A broken wrist is the second most common fracture in adults after the hip, and the most common fracture seen in people between the ages of 40 and 65. Most happen in a fraction of a second when someone instinctively throws out a hand to break a fall. The bone takes the full force of the fall so the head does not, and the distal radius, the lower end of the forearm bone closest to the wrist, snaps. What happens in the next 24 to 48 hours after that fracture determines whether you regain full wrist function or live with chronic pain, stiffness, and reduced grip strength for years.
The decisions made early matter enormously. Not every wrist fracture needs surgery. But some fractures that appear minor on first X-ray are unstable, will shift inside the medical plaster, and will heal in a malunited position unless treated surgically. Understanding which fracture you have, what treatment is appropriate for it, and what recovery requires is the difference between a wrist that returns to full function and one that does not.
The Anatomy Behind the Injury: Which Bone Usually Breaks
The wrist is made up of ten bones: the radius and ulna in the forearm, and eight small carpal bones in the wrist itself. When someone falls on an outstretched hand, the force travels through the palm into the radius. The radius, positioned on the thumb side of the forearm, absorbs the majority of the compressive load. According to the NIH StatPearls clinical reference on distal radius fractures, over 70% of wrist fractures involve the distal radius, specifically the last few centimetres before the wrist joint. This is the Colles’ fracture zone.
The scaphoid, a small carpal bone at the base of the thumb, is the second most commonly fractured wrist bone. Scaphoid fractures are notoriously easy to miss on initial X-ray, can look like a sprain for the first week, and carry serious complications if treated incorrectly. A wrist that remains painful and swollen more than a week after what appeared to be a sprain warrants repeat imaging or an MRI.
Types of Wrist Fractures and What Each Means for Treatment
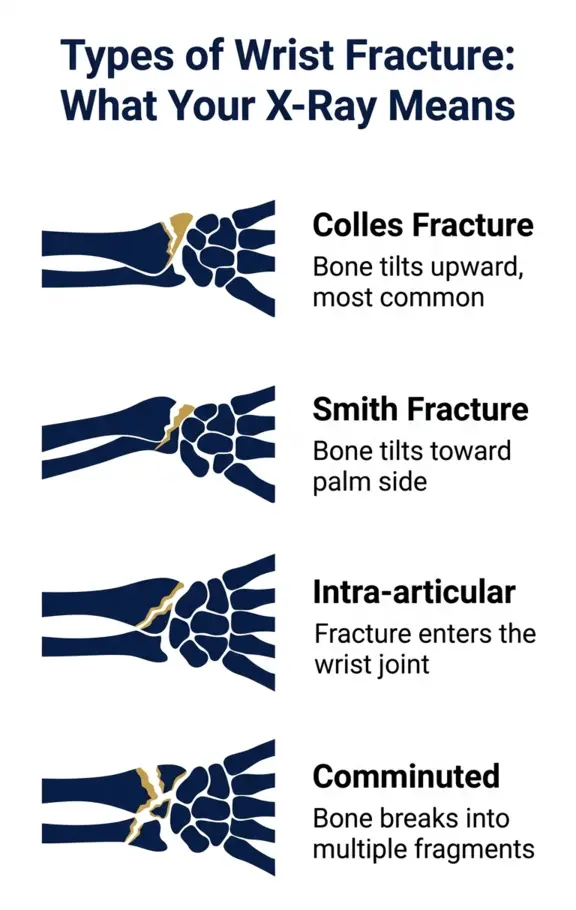
1. Colles’ Fracture
The classic wrist fracture. The distal radius breaks and the broken fragment tilts upward and backward, toward the back of the hand. From the side, the wrist profile takes on a distinctive dinner fork shape. Colles’ fractures are overwhelmingly the most common pattern, particularly in women over 50 and in patients with osteoporosis. They result from falling forward onto an outstretched hand with the wrist extended. Depending on displacement, instability, and whether the fracture involves the joint surface, Colles’ fractures are managed with medical plaster, closed reduction and medical plaster, or surgical plating.
2. Smith Fracture
The reverse of a Colles. The broken fragment tilts toward the palm rather than backward. Smith fractures result from falling backward onto a flexed wrist, or from a direct blow to the back of the wrist. They are less common than Colles but more frequently require surgery because the forward tilt of the fragment tends to be inherently unstable inside a medical plaster.
3. Barton Fracture
A fracture-dislocation where a piece of the articular surface of the radius breaks off and the wrist joint partially dislocates with it. Barton fractures virtually always require surgical fixation because the joint surface is disrupted and must be anatomically restored to prevent early post-traumatic arthritis.
4. Intra-articular Fractures
When the fracture line extends into the wrist joint surface itself, accurate restoration of the joint surface becomes critical. A large-scale epidemiological study published in BMC Musculoskeletal Disorders examining over 23,000 wrist fractures found that intra-articular fractures (AO-23-C type) had a 48% surgical rate compared to 18% for non-articular fractures. When the joint surface steps off by more than 2 millimetres, conservative medical plaster alone carries an unacceptably high risk of arthritis and long-term functional loss.
5. Comminuted Fractures
The bone shatters into multiple fragments rather than breaking cleanly in one or two places. Comminuted fractures are more common in high-energy injuries, in patients with severe osteoporosis, and in elderly patients with very fragile bone. They are technically more challenging to treat surgically but often require fixation precisely because the multiple fragments cannot be held reliably in a medical plaster.
6. Scaphoid Fractures
These deserve separate discussion. The scaphoid has a notoriously poor blood supply, particularly in its proximal portion. A fracture in the proximal third of the scaphoid that is not immobilised correctly, or goes undiagnosed, has a significant risk of avascular necrosis, where the bone fragment loses its blood supply and dies. A patient with persistent pain at the base of the thumb after a fall, even with a normal initial X-ray, should have an MRI of the wrist to rule out an occult scaphoid fracture. A missed scaphoid fracture treated as a sprain is one of the most consequential diagnostic errors in hand and wrist orthopaedics.
Medical Plaster vs Surgery: How the Decision Is Made
The treatment decision for a wrist fracture is not purely about which fracture type you have. It is made at the intersection of four variables: the fracture pattern on imaging, the degree of displacement, the patient’s age and bone quality, and the patient’s functional demands.
When Medical Plaster Works Well
Non-displaced or minimally displaced extra-articular fractures in patients with acceptable bone quality can be treated with a well-moulded below-elbow medical plaster for 5 to 6 weeks with regular X-ray monitoring. The monitoring component is critical: X-rays are taken at one week and two weeks after initial medical plaster application to confirm the position has not shifted. If the fracture redisplaces inside the medical plaster, surgical intervention is still possible and often preferable to accepting a malunited result.
Closed reduction, where the surgeon manipulates the bone back into alignment under local anaesthesia before applying the medical plaster, is appropriate for displaced but stable fractures where the reduction holds on repeated examination. Stability is assessed by the fracture geometry, the degree of comminution, and the patient’s bone quality.
When Surgery Gives Better Outcomes
Surgery becomes the recommended path when:
- The fracture is intra-articular with articular step-off greater than 2 mm
- The dorsal tilt after reduction exceeds 10 to 15 degrees and the fracture is unstable
- There is significant comminution that prevents the fracture from holding its position
- The initial closed reduction fails or the fracture redisplaces on follow-up X-ray
- The patient is young, working with their hands, or has high functional demands from sport or occupation
- The fracture is a Smith type or Barton fracture with inherent instability
A 2026 comparative study published in Nature Scientific Reports directly comparing medical plaster, external fixation, and volar plate fixation for distal radius fractures found that volar locking plate fixation produced superior early functional recovery and anatomical restoration, particularly for intra-articular fracture patterns. For displaced fractures, the functional advantages of surgical fixation over medical plaster application are measurable in grip strength, range of motion, and return to work timelines at 6 months.
Surgical Options for Wrist Fractures in Indore
Volar Locking Plate Fixation (ORIF)
The most commonly performed surgical technique for distal radius fractures in 2026, and central to minimally invasive wrist surgery at the clinic. The surgeon makes a small incision on the palm side of the wrist, carefully protects the flexor tendons and median nerve, positions the fractured bone fragments back into anatomical alignment under direct vision, and secures them with a low-profile titanium plate and locking screws. The plate sits against the front face of the radius, well away from the tendons that glide over the back of the wrist.
Volar plating allows early mobilisation within days to a week of surgery, significantly accelerating the recovery of grip strength and range of motion compared to medical plaster immobilisation for equivalent fractures. Patients can begin gentle wrist movement under physiotherapy guidance almost immediately, which prevents the joint stiffness that is one of the most disabling complications of prolonged medical plaster immobilisation.
Percutaneous K-Wire Fixation
Thin metal wires are passed through the skin under X-ray guidance to hold the reduced fracture fragments in place without a large open incision. K-wire fixation is less technically demanding than volar plating and works well for certain fracture patterns, particularly in younger patients with good bone quality and relatively simple fracture geometry. The wires are typically removed at 4 to 6 weeks once the bone has healed sufficiently.
External Fixation
A metal frame is applied to the outside of the arm, with pins passing through the skin into the bone above and below the fracture. External fixation holds the fracture through ligamentotaxis, using the tension of the wrist ligaments to maintain fracture alignment. It is used primarily for severely comminuted fractures, open fractures, or in situations where internal fixation is not possible due to fracture geometry or patient factors. External fixation has largely been superseded by volar locking plates for most fracture types in modern practice.
The Osteoporosis Connection Every Patient Must Understand
A wrist fracture in a woman over 50 that results from a simple fall from standing height is not just a bone injury. It is a warning signal.
A major study published in PMC examining over 180,000 female patients with distal radius fractures found that women who received osteoporosis evaluation and treatment after a wrist fracture had significantly lower rates of subsequent fractures, including hip fractures, which carry far greater morbidity and mortality than wrist fractures. Yet a significant proportion of surgeons managing wrist fractures do not routinely address the underlying bone quality that allowed the fracture to happen.
After the age of 50, a wrist fracture from a minor fall should trigger a bone mineral density (DEXA scan) assessment. Osteoporosis, defined as a T-score below minus 2.5, is present in approximately 40% of postmenopausal women. Treating the bone quality problem after a wrist fracture is as important as treating the fracture itself. A hip fracture costs orders of magnitude more in morbidity, surgical complexity, and recovery burden than a wrist fracture. The wrist fracture is the warning. Acting on it can prevent the hip fracture.
At Dr. Prince Orthopaedic and Joint Care Clinic, every patient over 50 with a low-energy wrist fracture is counselled on bone health assessment. The fracture is fixed. The underlying bone disease is not ignored.
Wrist Fracture Recovery Timeline: Realistic Expectations
Recovery timelines vary significantly by fracture type, age, and treatment method. These are the realistic benchmarks patients should plan around:
Conservative Treatment (Medical Plaster)
- Medical plaster worn for 5 to 6 weeks
- X-ray monitoring at weeks 1, 2, and 4 to confirm position
- After medical plaster removal: wrist will be stiff, grip strength significantly reduced
- Physiotherapy begins immediately after the medical plaster comes off
- Light activities of daily living: 6 to 8 weeks from injury
- Driving (with right wrist fracture): typically 6 to 8 weeks
- Return to desk work: 4 to 6 weeks with medical plaster support
- Return to manual labour or sport: 10 to 16 weeks
- Full grip strength recovery: 3 to 6 months
Surgical Treatment (Volar Plate)
- Surgery performed within 5 to 7 days of injury ideally, when swelling allows
- Wrist splint for 1 to 2 weeks post-surgery
- Physiotherapy begins at 5 to 7 days post-operatively
- Active wrist movement in physiotherapy by week 2
- Light activities of daily living: 2 to 3 weeks post-surgery
- Return to desk work: 2 to 4 weeks
- Return to manual work or sport: 8 to 12 weeks
- Full grip strength recovery: 3 to 4 months
The surgical recovery timeline advantage is most meaningful for patients who work with their hands, play sport, or have occupations that demand early return to full upper limb function.
What Happens If a Wrist Fracture Heals in the Wrong Position
Malunion, where the fracture heals with the bone in an incorrect alignment, is one of the most significant complications of wrist fracture management. It occurs when a displaced fracture is treated conservatively and shifts inside the medical plaster, or when the initial reduction was inadequate and not corrected in time.
A wrist that heals in malunion with more than 10 to 15 degrees of dorsal tilt typically results in:
- Permanent reduction in wrist flexion and extension range
- Chronic pain with forearm rotation
- Reduced grip strength, particularly for power tasks
- Altered biomechanics at the distal radioulnar joint causing ulnar-sided wrist pain
- Accelerated post-traumatic arthritis if the joint surface was disrupted
Correcting a malunion surgically, through a corrective osteotomy, is possible but significantly more complex than fixing the original fracture correctly. The lesson is consistent in orthopaedic literature: early, anatomical treatment of displaced or unstable wrist fractures prevents the complications that require far more difficult secondary procedures.
Physiotherapy After Wrist Fracture: The Phase That Determines Function
Whether treatment is conservative or surgical, the quality and consistency of post-fracture physiotherapy determines the final functional result more than any other single factor after the initial management.
The goals of wrist fracture physiotherapy progress through defined phases:
- Phase 1 (weeks 1 to 3 post-immobilisation or post-surgery): Oedema reduction, finger and shoulder active movement to prevent stiffness in adjacent joints, gentle assisted wrist movement within pain limits.
- Phase 2 (weeks 3 to 8): Progressive active and passive wrist flexion, extension, and rotation. Grip strengthening begins with soft putty. Scar management for surgical patients.
- Phase 3 (weeks 8 to 16): Functional strengthening, tool use, return to work tasks. Power grip and pinch strength training. Sport-specific movements for athletic patients.
Patients who begin physiotherapy promptly after the medical plaster comes off or surgery consistently achieve better functional outcomes than those who delay. Stiffness that sets in over the first 4 to 6 weeks after the medical plaster comes off without active physiotherapy can become permanent if not addressed early and consistently.
Post-fracture rehabilitation is available at Dr. Prince Orthopaedic and Joint Care Clinic’s rehabilitation programme.
Warning Signs After a Wrist Injury That Must Not Be Ignored
Not every wrist injury after a fall is immediately obvious in its severity. These symptoms, if present, indicate the injury needs same-day orthopaedic assessment and must not be managed as a sprain at home:
- Visible deformity or abnormal contour of the wrist
- Swelling that develops rapidly over 2 to 3 hours
- Numbness, tingling, or pins-and-needles in the fingers, particularly the thumb, index, and middle finger (suggests median nerve involvement from acute carpal tunnel compression)
- Inability to move the wrist or grip anything
- Persistent pain at the base of the thumb more than 5 to 7 days after injury even with normal initial X-ray (possible scaphoid fracture)
- Skin pallor, coldness, or abnormal capillary refill in the fingers after injury (emergency vascular assessment required)
Wrist Fracture Care at Dr. Prince Orthopaedic and Joint Care Clinic, Nipania, Indore
Wrist fractures and complex hand and wrist injuries are among the conditions managed at Dr. Prince Orthopaedic and Joint Care Clinic by Dr. Prince Uchadiya, DNB Orthopaedics Gold Medalist, trained at KEM Hospital, Mumbai. The clinic handles the full spectrum of wrist fracture management, from initial assessment and closed reduction to fracture and trauma management including volar plate surgery and post-operative rehabilitation.
Every patient’s imaging is reviewed personally by Dr. Prince. The treatment plan, whether conservative or surgical, is explained in full with the specific reasoning based on fracture pattern, displacement, and patient factors before any decision is confirmed. Patients coming from Bhopal, Ujjain, Ratlam, Dewas, Jabalpur, and across Madhya Pradesh for fracture management have access to the same standard of fellowship-trained specialist care as metro hospital centres at significantly lower cost.
Frequently Asked Questions: Wrist Fracture Treatment in Indore
1. How do I know if my wrist is fractured or just sprained?
A fracture causes rapid swelling within hours of injury, significant pain with any attempt to move the wrist, and usually a visible change in wrist contour. A sprain causes pain and bruising but the shape of the wrist remains normal and some movement is possible with discomfort. The only way to confirm a fracture is with X-ray. Any significant wrist injury after a fall should be X-rayed the same day. Do not assume it is a sprain because you can move the fingers: you can move your fingers with a fractured wrist. The wrist movement itself is what is restricted.
2. Does every wrist fracture need surgery?
Data from a large national fracture registry published in BMC Musculoskeletal Disorders found that 74% of distal radius fractures are treated non-surgically with medical plaster application. Surgery is needed when the fracture is displaced and unstable, when it involves the joint surface with a step greater than 2 mm, when it is a Smith or Barton pattern, or when medical plaster fails to hold the reduction on follow-up X-ray.
3. How long will I be in a medical plaster for a wrist fracture?
Standard medical plaster immobilisation for a distal radius fracture is 5 to 6 weeks. During this time, X-rays are taken at one week and two weeks to confirm the position has not shifted. If the position shifts, the medical plaster may be changed or surgery may become necessary.
4. What is volar plate surgery for a broken wrist?
Volar plate fixation, or open reduction and internal fixation (ORIF), involves making a small incision on the palm side of the wrist to directly see and restore the fracture alignment, then securing it with a low-profile titanium plate and locking screws. The plate holds the bone rigidly in correct position, allowing physiotherapy and movement to begin within days of surgery rather than waiting 6 weeks for the medical plaster to come off. The plate is usually left permanently in place, though occasionally it is removed after full healing if it causes discomfort from tendon irritation.
5. Is volar plate surgery done under general anaesthesia?
Wrist fracture surgery is typically performed under regional anaesthesia, specifically a brachial plexus block that numbs the entire arm, combined with sedation. General anaesthesia is used when regional block is not suitable. Most patients go home the same day or after one overnight stay.
6. When can I drive after a broken wrist?
With a left wrist fracture in an automatic car, patients who have had surgery often return to driving at 3 to 4 weeks when they have adequate grip and control. With a right wrist fracture or a manual gearbox, most surgeons advise waiting until at least 6 to 8 weeks after surgical fixation or after the medical plaster comes off. Always confirm with your surgeon before returning to driving, as individual recovery varies significantly.
7. Why does my wrist still hurt after the medical plaster comes off?
Pain, stiffness, and weakness after the medical plaster comes off are normal and expected. The joint has been immobilised for 5 to 6 weeks, the surrounding muscles have weakened, and the soft tissues around the wrist are stiff. This is precisely why physiotherapy begins immediately after the medical plaster comes off. The pain from disuse and stiffness resolves progressively with movement and strengthening over 6 to 12 weeks. Pain that worsens rather than improves, or new pins-and-needles in the fingers, warrants review with your treating orthopaedic surgeon.
8. I am 65 years old and broke my wrist in a fall at home. Should I be worried about my bones?
Yes, and your orthopaedic surgeon should be addressing this with you. A wrist fracture from a fall from standing height in a patient over 50 is classified as a fragility fracture, which is a strong indicator of reduced bone density. Research published in PMC demonstrates that patients who receive osteoporosis treatment after a wrist fracture have significantly lower rates of subsequent hip and vertebral fractures. Ask your doctor about a DEXA scan (bone mineral density test) and calcium and vitamin D supplementation. Treating the fracture without addressing the underlying bone health is an incomplete response to what may be a systemic bone disease.
9. Can a scaphoid fracture be missed?
Yes, frequently. Scaphoid fractures in the early days after injury can appear normal on plain X-ray in up to 20% of cases. The only reliable way to exclude a scaphoid fracture in a patient with snuffbox tenderness (pain at the base of the thumb near the wrist) is MRI of the wrist. A scaphoid fracture treated as a sprain that goes unimmobilised for 2 to 4 weeks has a significantly higher risk of non-union and avascular necrosis. If a fall on the hand left you with persistent pain specifically at the base of the thumb and your X-ray was reported as normal, ask your doctor explicitly whether a scaphoid fracture has been excluded with MRI.
10. How do I book a wrist fracture assessment in Indore?
Contact Dr. Prince Orthopaedic and Joint Care Clinic at the clinic contact page. Bring your X-rays or any imaging already done, along with the radiology report. For acute fractures, same-day or next-day appointments are prioritised. Dr. Prince will review your imaging personally, examine the wrist clinically, and give you a clear recommendation on whether medical plaster application, surgical reduction, or operative fixation is the right path for your specific fracture.
Medical Disclaimer: The information provided on this website is for general educational and informational purposes only and should not be considered medical advice. It is not intended to replace a consultation, diagnosis, or treatment by a qualified healthcare professional. If you are experiencing pain, injury, or symptoms, we strongly recommend consulting a qualified doctor for proper diagnosis and treatment. In case of a medical emergency, seek immediate medical attention.