
Hip dysplasia is one of those conditions that often goes unnoticed for years. A child born with a slightly shallow hip socket may walk fine until their twenties or thirties, when the joint slowly begins to break down and the pain starts creeping in. By the time most adults in Indore search for answers, they have already been told by two or three doctors that they have “hip pain” without anyone explaining the actual reason.
This page is about changing that. Whether you are a parent who just received a DDH diagnosis for your newborn, a young adult with unexplained groin pain, or someone in their40s whose hip has become a daily problem, understanding hip dysplasia treatment in Indore starts with understanding what is actually happening inside the joint.
What Hip Dysplasia Actually Is and Why It Matters
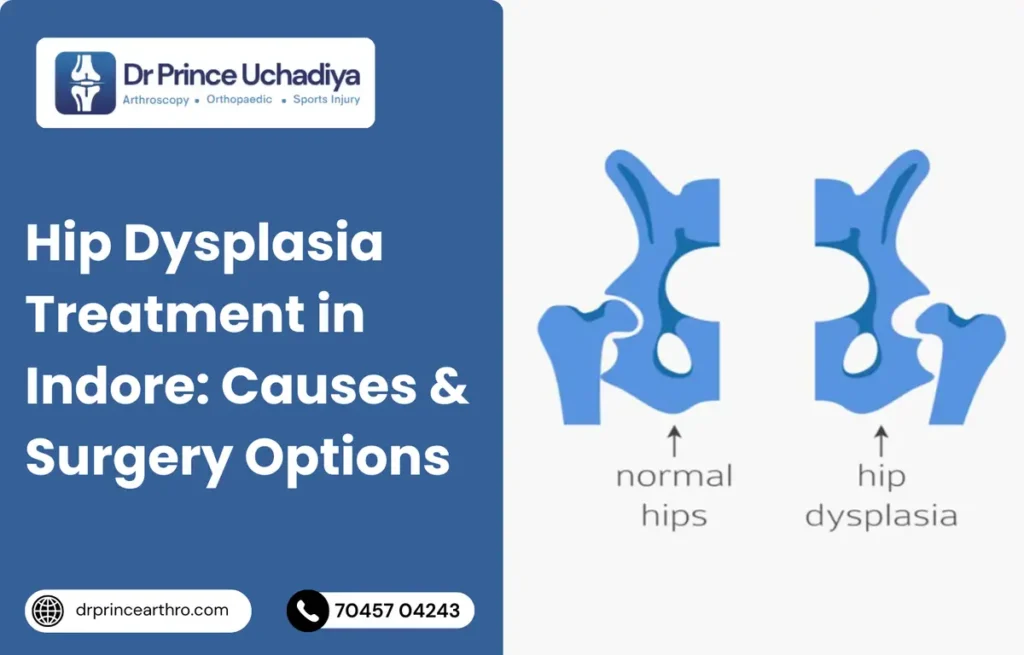
The hip is a ball-and-socket joint. The ball is the head of your femur (thigh bone), and the socket is called the acetabulum, a curved cup-shaped part of your pelvis. In a healthy hip, the socket covers the ball completely, distributing pressure evenly across the cartilage during every step you take.
In hip dysplasia, the socket is too shallow. It does not cover enough of the femoral head. This means the weight of your body is concentrated on a smaller area of cartilage, which wears down faster than it should. Over time, the labrum (a ring of cartilage around the socket edge) tears. The cartilage inside the joint degrades. Eventually, if left untreated, the joint develops severe arthritis.
What makes hip dysplasia particularly tricky is that it does not always cause obvious symptoms in childhood. Many people walk normally for decades before the joint begins to fail. According to the Cleveland Clinic, hip dysplasia is one of the leading causes of hip arthritis in people under 50 years of age, and a significant percentage of total hip replacements performed in younger adults are directly linked to undiagnosed or undertreated dysplasia.
Types of Hip Dysplasia: From Newborns to Adults
Hip dysplasia does not look the same at every age, which is why treatment must be tailored to the patient.
Developmental Dysplasia of the Hip (DDH) in infants and newborns is the most common form. In DDH, the hip socket has not formed correctly during fetal development. The ball may sit partially or completely outside the socket. Paediatricians check for this at birth using a physical test called the Barlow and Ortolani manoeuvre. If caught within the first few weeks of life, it can usually be treated without surgery using a soft brace called a Pavlik harness.
Hip dysplasia in older children and adolescents is more complex. As the bones have started to harden, conservative bracing is often no longer effective. Surgical correction of the socket position becomes necessary.
Adult hip dysplasia is the form that most patients presenting to orthopaedic clinics in Indore are dealing with. This is either a mild form of DDH that was never detected, or dysplasia that developed gradually. The hallmark is chronic groin or hip pain that worsens with activity, often accompanied by a labral tear.
Symptoms That Tell You Something Is Wrong With Your Hip Joint
Hip dysplasia does not announce itself loudly. Most patients describe a slow, progressive pattern that they initially ignored, attributing the pain to muscle strain, gym injury, or just “getting older.”
The symptoms to watch for include:
- Pain in the groin or outer hip, especially after walking, running, or sitting for long periods
- A clicking, locking, or catching sensation inside the hip joint
- Hip stiffness after waking up or after periods of rest
- One leg appearing slightly shorter than the other
- A limp that has gradually worsened over months or years
- Pain that improves with rest but returns quickly with any physical activity
- Difficulty sitting cross-legged or squatting deeply
Many patients with hip dysplasia in Indore come to the clinic after months of physiotherapy that gave only partial relief. If physiotherapy is not improving your hip pain, the underlying structural problem of the socket needs to be evaluated.
Who Is at Higher Risk for Hip Dysplasia in India
Certain groups are more likely to develop hip dysplasia, and awareness of these risk factors can help with earlier detection.
Girls are significantly more affected than boys. Roughly one in 600 female babies is diagnosed with DDH, compared to one in 3,000 males. The reason is partly hormonal: the maternal hormone relaxin, which loosens the mother’s ligaments for childbirth, also affects the baby’s hip ligaments, and girls are more sensitive to this effect.
A family history of hip dysplasia increases the risk considerably. If a parent or sibling has had DDH, screening of newborns is strongly recommended. Being the firstborn child also slightly increases risk, as the uterus is tighter and the baby has less room to move, which can affect hip positioning.
Babies born in a breech position (feet first) have a much higher rate of hip dysplasia because the femoral head is not pressing correctly into the acetabulum during the critical period of socket formation in the womb. Tight swaddling with the legs straight has also been linked to higher DDH rates in some traditional practices.
How Hip Dysplasia Is Diagnosed in Indore
Getting an accurate diagnosis is the most important first step. At Dr. Prince Uchadiya Orthopaedic and Joint Care Clinic in Indore, the diagnostic process for hip dysplasia involves a combination of clinical examination and imaging.
During the physical examination, your doctor will test the range of motion of your hip, check for any leg length discrepancy, and perform specific provocation tests to reproduce your pain and identify its source. In infants, the Barlow and Ortolani tests are used to detect instability.
Imaging plays a central role:
- X-rays: The first and most important investigation. X-rays of the pelvis and hip, taken in specific positions, allow measurement of the lateral centre-edge angle (LCEA), which tells the surgeon exactly how much of the femoral head is covered by the acetabulum. An angle below 20 degrees is considered dysplastic.
- MRI: An MRI is ordered when a labral tear is suspected alongside the dysplasia. It gives detailed information about the cartilage, labrum, and surrounding soft tissues, which is critical for surgical planning.
- CT scan: Used in complex cases to understand the three-dimensional shape of the hip socket before major reconstructive surgery.
One of the most common mistakes made by patients searching for hip dysplasia treatment in Indore is receiving an MRI without proper X-ray measurement of socket coverage. The X-ray angles matter enormously in deciding which surgery is appropriate.
Hip Dysplasia Treatment in Infants: The Earlier, The Simpler
For newborns and infants below six months, the Pavlik harness is the standard first-line treatment. This soft fabric brace holds the baby’s hips in a flexed and abducted position, encouraging the femoral head to sit properly in the socket while the cartilage is still soft and moldable. The harness is worn for several weeks to months, with regular ultrasound monitoring to track socket development.
When the Pavlik harness fails or the diagnosis is made after six months, closed reduction under general anaesthesia is performed. The surgeon manipulates the hip into place without opening the joint and then places the child in a spica cast (a full pelvis and leg cast) to hold the position while the joint stabilizes. A period of four to six weeks in the cast is typical before imaging confirms adequate coverage.
Open reduction surgery becomes necessary when closed reduction cannot achieve satisfactory positioning. This involves surgically opening the joint, removing any tissue blocking the socket, and repositioning the femoral head. In older toddlers and children, bone reshaping procedures around the pelvis or femur are combined with the reduction to improve socket coverage.
Hip Dysplasia Surgery Options for Teenagers and Young Adults in Indore
This is where the management of hip dysplasia becomes most nuanced, and where choosing an experienced orthopaedic surgeon in Indore makes the biggest difference to your long-term outcome.
Periacetabular Osteotomy (PAO) is the gold standard surgery for hip dysplasia in skeletally mature adolescents and adults up to approximately 40 years of age where the cartilage is still intact or minimally damaged. In a PAO, the surgeon makes precise cuts around the hip socket and repositions it to better cover the femoral head, then fixes it with screws. The result is a more normal hip biomechanics that dramatically slows or prevents the development of arthritis.
The key advantage of PAO is that it preserves your own joint. Rather than replacing the hip with an artificial implant, it corrects the underlying cause. Research published on PubMed shows that PAO achieves excellent long-term outcomes in well-selected patients, with many avoiding hip replacement for 20 or more years after surgery.
PAO is not appropriate for everyone. Patients with significant cartilage loss or established arthritis may not benefit from joint preservation surgery. In those cases, total hip replacement becomes the more appropriate option.
Hip Arthroscopy is a minimally invasive procedure used to treat labral tears, remove loose tissue, and address cartilage damage inside the joint. When hip dysplasia causes a labral tear, hip arthroscopy can repair the torn labrum and reduce pain. However, arthroscopy alone does not correct the underlying socket shallowness, so it is often combined with PAO or used selectively in milder forms of dysplasia where the structural problem is not severe.
Femoral Osteotomy is sometimes performed alongside PAO when the angle of the femoral neck is contributing to the problem. The femur is cut and repositioned to improve how the ball sits within the newly positioned socket.
When Total Hip Replacement Becomes the Right Choice
For patients in Indore who are older or have advanced joint degeneration, total hip replacement is often the most effective path to a pain-free life. This is particularly true when:
- The cartilage inside the joint has been largely destroyed
- Significant arthritis has developed secondary to the dysplasia
- The patient is above 50 to 55 years of age
- Conservative treatments have failed to provide adequate pain relief
Hip replacement for dysplasia is technically more complex than standard replacement surgery because the socket is abnormally shaped. An experienced orthopaedic surgeon must carefully plan the positioning of the artificial acetabular cup to restore correct biomechanics. When done well, modern hip replacements provide excellent function and last 20 or more years in most patients.
A concern patients often raise is whether they are too young for hip replacement. The answer depends on the degree of joint damage, not the age on paper. An active 45-year-old with destroyed cartilage and daily debilitating pain will have a better quality of life with a well-performed hip replacement than with years of pain management and physiotherapy that provide diminishing returns.
Non-Surgical Management: Who It Works For and Who It Does Not
Not every patient with hip dysplasia needs surgery. In mild forms with minimal symptoms, a programme of targeted physiotherapy, activity modification, and anti-inflammatory management can keep pain controlled for years. The goal of non-surgical treatment is not to correct the structural problem but to reduce stress on the joint and strengthen the muscles that support it.
Non-surgical management works best for:
- Patients with very mild dysplasia and intact cartilage
- Older patients whose activity requirements are lower
- Patients who are not ready or fit for surgery
- Those using conservative care as a temporary measure while preparing for surgery
It is important to understand that physiotherapy, pain medication, and lifestyle changes do not stop the underlying joint deterioration in moderate to severe hip dysplasia. They manage symptoms. Delaying appropriate surgical correction when it is indicated often means the cartilage damage worsens, making surgery more complex and outcomes less predictable.
Hip Dysplasia Treatment Cost in Indore
Cost is a real and legitimate concern for families seeking hip dysplasia treatment in Indore. The range varies depending on the type of treatment required, the facility, and whether general or spinal anaesthesia is used.
Here is a general guide to what patients can expect:
- Pavlik harness (infants): Relatively affordable, typically between Rs. 3,000 to Rs. 8,000 for the brace itself, plus follow-up consultation and ultrasound monitoring costs.
- Closed reduction and spica cast: This requires a short hospital stay under anaesthesia. Total cost including hospitalisation typically ranges from Rs. 40,000 to Rs. 90,000.
- Hip arthroscopy for labral tear: Minimally invasive arthroscopic surgery for the hip in Indore ranges approximately from Rs. 70,000 to Rs. 1,50,000 depending on the complexity of the repair and hospital facility.
- Periacetabular Osteotomy (PAO): This is a major reconstruction surgery requiring a few days of hospitalisation and a longer recovery. In India, PAO surgery typically costs between Rs. 2,00,000 to Rs. 4,00,000 depending on the implants used, hospital tier, and surgical complexity.
- Total Hip Replacement: For patients with advanced dysplasia and arthritis, total hip replacement in Indore ranges from Rs. 2,50,000 to Rs. 5,50,000 for standard implants. Premium ceramic-on-ceramic implants add to this cost. Many patients are surprised to learn that hip replacement for dysplasia is covered under the Ayushman Bharat PM-JAY scheme for eligible patients.
At the time of consultation, the clinic will provide a transparent, itemised cost estimate based on your specific diagnosis and treatment plan. There are no hidden charges. The team will also help you understand any insurance or government scheme benefits you may be entitled to.
Recovery After Hip Dysplasia Surgery: What the Timeline Looks Like
Recovery timelines vary significantly depending on the surgery performed.
After hip arthroscopy, most patients are walking with support the same day or the next morning. Crutches are used for one to three weeks. Return to office work typically happens within two to three weeks, and full physical activity at three to four months.
After PAO surgery, the recovery is longer because the bones need to heal at the osteotomy sites. Patients typically stay in hospital for three to five days. Partial weight bearing with crutches continues for six to eight weeks. Most patients return to driving at six to eight weeks and to full activity at six to twelve months. Physiotherapy is essential throughout the recovery and is supervised by the in-house team at the clinic.
After total hip replacement, patients begin walking with support the day after surgery. Hospital discharge usually happens within two to three days. Most patients walk without a cane by six to eight weeks and return to low-impact activity by three months. Hip precautions (avoiding certain positions that risk dislocation) are followed during the first three months.
Dr. Prince Uchadiya’s Perspective on Hip Dysplasia: What He Tells Every Patient
Dr. Prince Uchadiya, Gold Medalist orthopaedic surgeon trained at KEM Hospital Mumbai and one of Indore’s most trusted specialists in arthroscopy, joint preservation, and hip replacement, shares his candid view on hip dysplasia:
“The biggest problem I see with hip dysplasia in Indore is not the condition itself. It is the delay. Patients come to me after three or four years of being told their pain is muscular or that they are too young to have a joint problem. By the time we get the right X-ray measurement, the labrum is already torn and in some cases the cartilage is damaged beyond what a preservation surgery can fix.
If you are under 40, have groin pain that does not go away, and your MRI says ‘labral tear,’ please ask your doctor to also measure the lateral centre-edge angle on your X-ray. That number tells us whether the socket is shallow. If it is below 20 degrees, that is hip dysplasia until proven otherwise.
The other thing I tell every young patient is this: surgery is not the enemy. Delaying the right surgery is the enemy. A PAO done early, when the cartilage is intact, gives you decades of your own natural joint. A total hip replacement done later is also excellent, but your own joint is always the better option for as long as it remains viable. My job is to identify which option gives you the longest and best quality of life, and then to perform it with precision.”
Dr. Prince Uchadiya’s approach at his Orthopaedic and Joint Care Clinic in Nipania, Indore combines detailed preoperative planning, modern minimally invasive surgical techniques, and structured post-operative rehabilitation to give every hip dysplasia patient the best possible long-term result.
10 Most Asked Questions About Hip Dysplasia Treatment in Indore
1. Can hip dysplasia be treated without surgery in adults?
In mild cases with no labral tear and minimal symptoms, physiotherapy and activity modification can manage symptoms for years. However, hip dysplasia with a shallow socket does not self-correct in adults. If the structural problem is moderate to severe and causing pain, surgery provides a more durable solution than non-surgical management alone. The question is not whether surgery can be avoided forever, but whether delaying it is causing more damage.
2. I was told I have a labral tear. Could it be caused by hip dysplasia?
Absolutely yes. Labral tears in young adults, especially women under 40, are frequently caused by hip dysplasia. When the socket is too shallow, the labrum takes on extra load to compensate and eventually tears. An MRI showing a labral tear should always prompt an X-ray measurement of socket coverage. Treating the labral tear without addressing the dysplasia often leads to the tear recurring.
3. My baby was diagnosed with DDH at birth. Will they need surgery?
Not necessarily. If DDH is caught within the first six weeks of life, a Pavlik harness resolves the problem in the majority of cases without any surgery. The earlier the diagnosis and treatment begin, the higher the chance of a completely normal outcome. Regular follow-up with ultrasound monitoring is essential during treatment.
4. What is the difference between hip dysplasia and hip impingement (FAI)?
These are opposite conditions. In hip dysplasia, the socket is too shallow and provides too little coverage. In femoroacetabular impingement (FAI), there is too much bone causing the ball and socket to pinch. Both can cause labral tears and groin pain, but they require different surgical approaches. An experienced hip surgeon will distinguish between them based on X-ray measurements and clinical examination.
5. Is PAO surgery available in Indore?
PAO requires a surgeon with specific training in hip preservation surgery and detailed preoperative planning. At Dr. Prince Uchadiya’s clinic in Indore, patients are assessed individually to determine whether they are candidates for joint preservation versus joint replacement. The appropriate surgery is recommended based on the patient’s age, cartilage status, and specific measurements.
6. How long does hip dysplasia surgery take, and how many days in hospital?
Hip arthroscopy typically takes one to two hours and patients go home the same day or the next morning. PAO surgery takes two to three hours and requires three to five days in hospital. Total hip replacement takes one to two hours with a two to three day hospital stay. Recovery at home with physiotherapy support follows each procedure.
7. Is hip replacement covered under Ayushman Bharat in Indore?
Yes, total hip replacement is included in the list of procedures covered under the Ayushman Bharat PM-JAY scheme, subject to the patient holding a valid Ayushman Bharat card and the hospital being empanelled under the scheme. Patients are advised to confirm coverage and eligibility directly with the clinic before proceeding.
8. At what age is it too late to have hip dysplasia corrected?
There is no absolute upper age limit. PAO is generally most appropriate for patients up to their late thirties or early forties with intact cartilage. Beyond this, or when significant arthritis is present, total hip replacement becomes the more appropriate surgery. Age alone does not determine the right treatment; the condition of the cartilage and the patient’s overall health matter more.
9. Will I walk normally after hip dysplasia surgery?
The goal of all hip dysplasia surgery is to restore normal, pain-free walking. Most patients who had a noticeable limp before surgery find that it improves significantly after appropriate treatment and physiotherapy. Full recovery of gait can take several months, particularly after PAO, but the majority of patients report dramatically improved function compared to before surgery.
10. How do I know if my hip pain in Indore is from dysplasia and not arthritis or a muscle problem?
The only way to know for certain is through a proper clinical examination combined with X-ray measurement of the hip socket and, if needed, an MRI. Pain location (groin versus outer hip), age of onset, and specific provocative tests help the orthopaedic surgeon differentiate dysplasia from other causes. If you are under 45 and have persistent groin pain not responding to physiotherapy, a dedicated hip assessment measuring socket coverage is worth requesting.


