
Many patients who have hip impingement do not know they have it.
They think it is a groin strain. Or a muscle pull. Or just the way they sit.
So they stretch it, ignore it, and carry on. Months pass. The pain becomes a background noise they have learned to live with.
Then one day the hip starts locking. Or they cannot climb stairs without wincing. Or a sports injury pushes things over the edge and the MRI finally shows the real problem.
Femoroacetabular impingement, also called FAI or hip impingement, is one of the most commonly missed causes of hip and groin pain in young and active adults in Indore.
This article explains everything you need to know, in plain language, so you can understand what is happening in your hip, what your options are, and when you actually need to act.
What Is Femoroacetabular Impingement (FAI)?
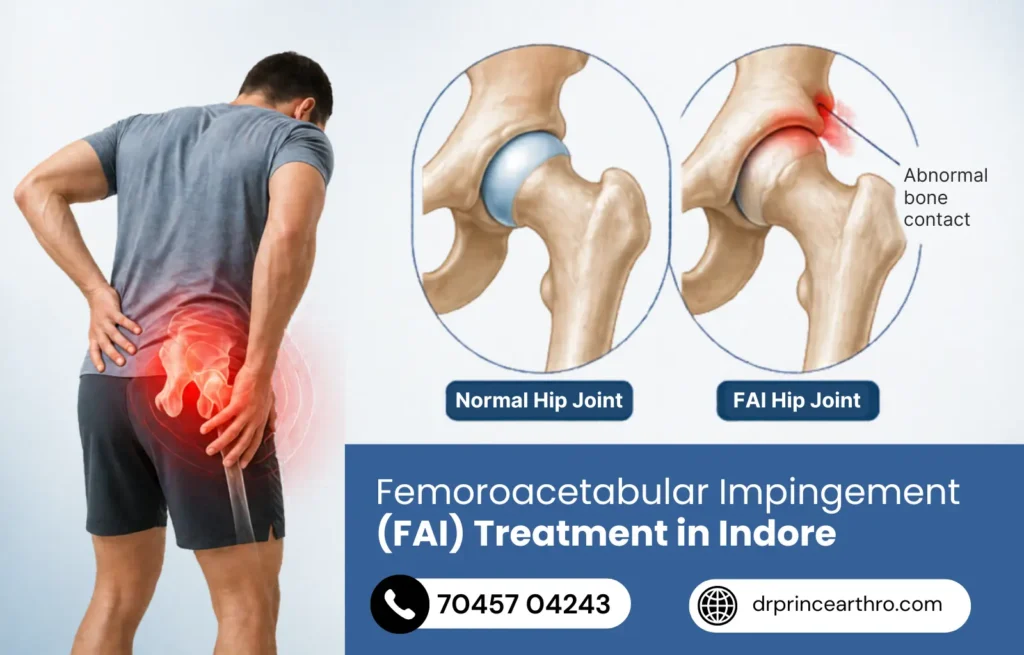
Your hip is a ball-and-socket joint. The ball is the rounded top of your thighbone (femoral head). The socket is the cup-shaped cavity in your pelvis (acetabulum).
In a healthy hip, the ball moves smoothly inside the socket in all directions. The surfaces are coated in slippery cartilage, and a ring of fibrocartilage called the labrum lines the rim of the socket to deepen it and improve stability.
In FAI, either the ball is not perfectly round, or the socket has grown too deep, or both. This means that when you move your hip into certain positions, especially deep bending and rotation, the bones pinch against each other instead of gliding smoothly.
Over time, that pinching damages the labrum and the cartilage underneath it. Left long enough, it accelerates joint degeneration and can lead to early-onset hip osteoarthritis.
This is not a disease that develops overnight. It builds up over years, which is exactly why it gets missed so often.
How Common Is FAI? The Numbers People Do Not Expect
FAI is far more common than most people realize.
According to research published in NCBI StatPearls, the prevalence of femoroacetabular impingement in the general adult population is between 10 to 15%.
In athletes, that number rises significantly. Symptomatic FAI has been reported in up to 55% of athletic populations.
Here is what makes it complicated: cam deformity (one of the two main FAI types) is found in 37% of completely asymptomatic people on imaging. Many people have the bony shape that causes impingement but never develop symptoms.
What pushes someone from “asymptomatic cam morphology” to “symptomatic FAI” is usually a combination of the severity of the bony abnormality, activity level, and how much cartilage and labral damage has accumulated over time.
So if you play sport in Indore, or had an active childhood with heavy loading on the hips, and now have groin or hip pain in your 20s or 30s, FAI deserves serious consideration.
The 3 Types of FAI: Cam, Pincer, and Mixed
Understanding which type of impingement you have matters for treatment planning.
Cam Impingement
This is when the femoral head (ball) is not perfectly round. It has a bony bump, usually at the front and outer part of the femoral neck, called a cam lesion.
When you bend the hip, this non-round surface jams against the rim of the socket, grinding the cartilage and tearing the labrum from the inside out.
Cam impingement is more common in men.
It is strongly linked to high-intensity sport during adolescence, particularly activities involving deep hip flexion and rotation like football, kabaddi, cricket (wicket-keepers), wrestling, and cycling.
Cam deformity prevalence in athletes is 54.8%, compared to just 23.1% in non-athletes. The growth plate of the femoral head is vulnerable during the teenage years, and repetitive stress during this period may alter how the head forms.
Pincer Impingement
This is when the socket (acetabulum) over-covers the femoral head. The rim of the socket extends too far, so the labrum gets crushed between the rim and the femoral neck every time you bend your hip.
Pincer impingement is more common in women.
The damage pattern here is different from cam. The labrum takes the direct hit first, with cartilage damage developing more gradually behind it.
Mixed (Combined) Impingement
This is by far the most common type, present in roughly 70-73% of FAI cases in large series. Most patients have elements of both cam and pincer morphology, which typically produces more complex joint damage and needs careful surgical planning.
FAI Symptoms: What It Actually Feels Like Day to Day
The classic FAI patient in Indore describes their symptoms in one of these ways:
“I get a deep ache in my groin, especially after sitting for a long time.”
“My hip hurts when I go up stairs or get out of a car.”
“When I bend forward in yoga or squat at the gym, there is a sharp pinching sensation in the hip.”
“I feel stiffness in the hip first thing in the morning that takes time to ease.”
These are the hallmarks. Let us break them down properly.
- Deep groin pain, often described as being “inside” the hip rather than on the surface
- Pain in the front of the hip, the groin, and sometimes the outer thigh
- Stiffness and reduced range of motion, particularly in bending and rotating the hip inward
- Pain that is worse with prolonged sitting, especially in low chairs or car seats
- Sharp catching or pinching pain at the end range of hip bending and rotation
- Clicking or locking of the hip in some positions
- Pain that radiates into the buttock or lower back in some cases
The “C-sign” is a classic clinical finding. Ask a patient with FAI where their pain is, and they will often cup their hand in a C-shape around the side of their hip, placing the thumb on the back and fingers on the groin. That instinctive gesture maps the location of the impingement. It is something we specifically look for in the clinic.
The FADIR Test: How FAI Is Diagnosed on Examination
The most reliable physical test for femoroacetabular impingement is called the FADIR test: Flexion, Adduction, Internal Rotation.
The patient lies flat. The examiner bends the hip to 90 degrees, then brings the knee across the midline (adduction), then rotates the foot outward (internal rotation of the hip).
In FAI, this position reproduces the exact mechanism of impingement. The femoral neck collides with the acetabular rim. The test is positive when it recreates the patient’s familiar deep hip or groin pain.
The FADIR test has high sensitivity for FAI, meaning most patients with FAI will test positive. However, sensitivity alone does not make a diagnosis. A positive FADIR combined with imaging findings and a clear symptom history is what gives a confident FAI diagnosis.
Imaging typically involves X-rays of the pelvis to assess the bony morphology, including measurement of the alpha angle on the femoral head. An alpha angle greater than 50-55 degrees indicates a cam deformity. MRI or MR arthrography adds information about labral tears and cartilage damage, which are the consequences of the impingement.
What Happens If FAI Is Left Untreated
This is the part that changes how most patients think about FAI.
FAI is not a condition you can simply modify your way out of permanently. The bony abnormality is structural. It does not go away with stretching, rest, or lifestyle changes.
What conservative treatment does is reduce symptoms and slow the progression of damage. It does not correct the underlying impingement mechanism.
Every time the hip moves into the impingement position, the labrum and cartilage take a hit. Small hits accumulate into bigger damage over months and years.
Untreated FAI leads to:
- Progressive labral tears that grow from small partial tears into full circumferential tears
- Cartilage damage that cannot be reversed once established
- Early-onset hip osteoarthritis, often before age 50
- In severe cases, the need for total hip replacement at an age that would otherwise never have been necessary
Research consistently identifies FAI as one of the leading causes of early hip osteoarthritis in young adults. Cam-type FAI in particular carries a clear evidence link to progressive joint degeneration.
This is why the timing of treatment matters. A labrum that can be repaired today may be irreparable in two years. A cartilage surface that is intact today may develop deep lesions if the impingement continues unchecked.
Early assessment and appropriate intervention protects the joint. Delay narrows the options and worsens outcomes.
Non-Surgical Treatment for FAI in Indore: What Works and What Does Not
For many patients, especially those with mild symptoms and no significant labral or cartilage damage, conservative management is the appropriate starting point.
Conservative treatment for femoroacetabular impingement treatment in Indore includes:
Activity Modification
Identifying and reducing the movements that provoke impingement. This does not mean stopping activity entirely. It means smart modification.
Deep squats, high kicks, cycling with a low saddle, tight hip flexion in yoga, and sitting cross-legged on the floor are the main offenders. These can often be adjusted or temporarily avoided without eliminating exercise altogether.
Targeted Physiotherapy
Not generic hip stretches. The physiotherapy approach for FAI focuses on strengthening the muscles around the hip, particularly the gluteus medius, deep hip rotators, and core stabilizers, to reduce the mechanical load on the impinging region.
The goal is to improve movement patterns so the hip operates further away from the impingement zone during daily activities and exercise.
Research shows that well-structured physiotherapy can meaningfully reduce pain and improve function, particularly in patients with milder morphology and early-stage labral involvement.
Anti-Inflammatory Medication
NSAIDs help manage the inflammatory response around an irritated labrum and joint capsule. They reduce pain during activity and aid sleep. They do not treat the underlying impingement but are an important part of the symptom management package.
Intra-Articular Injection
A corticosteroid injection directly into the hip joint can provide significant short-term relief, typically lasting weeks to months. It is also used diagnostically, because if an intra-articular injection takes the pain away, it confirms the pain is coming from inside the joint rather than from surrounding muscles or tendons.
Injections are useful for patients who need temporary relief to engage in physiotherapy or who are waiting for surgery.
The Honest Limitation of Conservative Treatment
Studies comparing conservative management to surgery for FAI show that surgery tends to produce better outcomes at the one-year mark. By two years, outcomes are similar in patients with milder disease. But in patients with significant labral tears or cartilage damage, conservative treatment does not repair the structural injury. It manages symptoms while the underlying problem continues.
This is the clinical reality: conservative treatment is an excellent first step for mild to moderate FAI. It is not a permanent solution for patients with structural damage that needs repair.
Hip Arthroscopy for FAI in Indore: What the Surgery Involves
When conservative management has not provided enough relief, or when the labral tear or cartilage damage is significant enough to warrant direct treatment, hip arthroscopy for FAI is the surgical standard of care.
It is a minimally invasive procedure. Two to three small incisions, each just a few millimetres, allow a camera and fine surgical instruments to enter the hip joint.
What gets done inside the joint depends on what is found:
- Cam resection (femoroplasty): The bony bump on the femoral neck is carefully shaved down to restore the normal round shape of the femoral head. This removes the source of the impingement mechanically.
- Pincer resection (acetabuloplasty): The over-prominent rim of the acetabulum is trimmed back to reduce socket over-coverage.
- Labral repair: Where the labrum is torn but still has viable tissue, it is reattached to the acetabular rim with small suture anchors. Preserving the labrum is always preferable to removing it, because the labrum contributes to hip stability and joint fluid pressure.
- Labral debridement: Where labral tissue is too damaged to repair, the frayed portion is carefully trimmed.
- Cartilage treatment: Damaged cartilage areas may be smoothed (chondroplasty) or, for deeper lesions, treated with microfracture to stimulate fibrocartilage formation.
The entire procedure usually takes 60 to 90 minutes. It is done under general or spinal anaesthesia. Most patients go home the same day or the following morning.
You can learn more about how we approach arthroscopic surgery at our Indore clinic, including what patients typically experience before and after the procedure.
FAI Surgery Results: What the Evidence Says
The outcomes from hip arthroscopy for FAI are well-documented and encouraging.
Studies show that 85 to 90% of patients who undergo hip arthroscopy for FAI return to sports and physical activities at the level they were at before their hip pain began.
According to Cleveland Clinic, surgery to repair femoroacetabular impingement has a very high success rate when performed at the right stage of the disease.
The complication rate for hip arthroscopy is approximately 1.7%, which is very low for a joint surgical procedure. The re-operation rate is around 5.5%.
The key caveat in all these numbers is timing. Outcomes are significantly better when surgery is performed before advanced cartilage damage has occurred. Patients with large areas of full-thickness cartilage loss have less predictable results because the cartilage cannot be regenerated.
This is why “watch and wait” for years is not always the conservative approach it sounds like. It can be the approach that costs you the best surgical outcome.
FAI Surgery Recovery: Week by Week
Recovery after hip arthroscopy for FAI is longer than knee arthroscopy. The hip is a deeper joint with a more complex capsule, and the repair of labral tissue requires protection during healing.
Week 1 to 2
Crutches are used to protect the operated hip. Weight-bearing is partial and carefully graded. Pain is managed with anti-inflammatories and ice. Gentle range-of-motion exercises begin almost immediately to prevent stiffness.
Week 2 to 6
Physiotherapy begins in earnest. Focus is on restoring range of motion, activating the hip stabilizers gently, and progressing weight-bearing. Most patients are walking without crutches by week 4 to 6.
Week 6 to 12
Progressive strengthening. Stationary cycling begins. Pool walking and swimming are typically well tolerated. Return to desk work for most patients is in this window.
Month 3 to 4
Jogging begins on flat ground. Functional movement patterns that mimic sport are introduced under physiotherapy supervision.
Month 4 to 6
Return to non-contact sport and physical activity for most patients. Full return to competitive sport, particularly for athletes requiring high-demand hip movement, typically takes 6 to 9 months.
Patients sometimes feel frustrated by the length of recovery compared to other arthroscopic procedures. The important context is that labral tissue repaired with suture anchors needs 12 to 16 weeks to achieve adequate healing strength. Pushing through this phase risks re-tearing the repair and losing the benefit of surgery.
FAI in Young Athletes from Indore: A Specific Risk Profile
Indore has a large and growing population of young athletes in cricket, football, kabaddi, wrestling, and gym-based sports. All of these involve repetitive deep hip loading.
Cricket wicket-keepers spend years in deep squatting positions. Wrestlers and kabaddi players load the hip through extreme ranges repeatedly. Football players perform thousands of pivoting, cutting, and kicking movements every season. Regular gym-goers doing heavy squats and deadlifts load the femoral neck continuously.
All of these activities are not causes of FAI by themselves, but they are significant accelerants. If the underlying bony morphology is there and the activity loads it repeatedly, the cartilage and labrum accumulate damage faster.
The most important thing for young athletes in Indore is to get assessed early if groin or hip pain has been present for more than 4 to 6 weeks. At that stage, the options are widest and the recovery from any intervention is fastest.
FAI vs. Other Hip Conditions: Getting the Diagnosis Right
Several conditions mimic FAI symptoms and can lead to confusion or incorrect treatment if the diagnosis is not properly established.
The main differential diagnoses that need to be considered alongside FAI include:
- Hip labral tear without FAI: Labral tears can occur from other mechanisms including hypermobility and trauma. FAI is the most common cause but not the only one.
- Iliopsoas tendinopathy: A tight or irritated iliopsoas tendon causes pain at the front of the hip with hip flexion. It is often confused with FAI but responds differently to treatment.
- Adductor muscle strain: Groin pain that is point tender along the inner thigh rather than deep in the joint suggests muscle injury rather than intra-articular pathology.
- Hip osteoarthritis: In older patients, established arthritis may coexist with or mimic FAI. An X-ray showing significant joint space narrowing changes the treatment direction considerably.
- Stress fracture of the femoral neck: In young athletes with hip pain, a stress fracture must be ruled out, particularly if the pain is worse with impact activities and the athlete trains at high volumes.
Accurate diagnosis is the foundation of effective treatment. The physical examination, the nature and location of symptoms, and a properly reviewed set of imaging studies together build the clinical picture. No single test makes the diagnosis alone.
Why Patients in Indore Choose Dr. Prince Uchadiya for FAI Treatment
Hip arthroscopy for femoroacetabular impingement is a technically demanding procedure. The hip is a deeper joint than the knee, with less natural space to work in. The precision of the bone resection matters, because under-resection leaves the impingement uncorrected, and over-resection weakens the femoral neck.
Dr. Prince Uchadiya is a gold medalist orthopedic surgeon with postgraduate training from KEM Hospital, Mumbai, and subspecialty expertise in arthroscopy, ligament reconstruction, and minimally invasive joint preservation. His approach to FAI mirrors his approach to every musculoskeletal condition: conservative first, surgical when the clinical evidence supports it, and always guided by the long-term health of the joint.
Patients from Vijay Nagar, Nipania, Palasia, Bengali Square, Mahalaxmi Nagar, and across Indore consult the clinic for hip pain evaluation, FAI diagnosis, and both non-surgical and arthroscopic treatment.
For a broader look at the clinic’s philosophy and range of services, visit the Dr. Prince Uchadiya Orthopaedic And Joint Care Clinic homepage.
Dr. Prince Uchadiya on FAI: What He Tells Patients in Clinic
FAI is a condition that I find particularly satisfying to treat, because when it is caught at the right time and managed correctly, young people get their active lives back completely. A 24-year-old who was struggling to play football in Indore can be back on the field in 6 to 9 months with a hip that moves properly again. That outcome is worth a great deal.
The challenge is that FAI gets missed for too long. Patients come in having been told it is a muscle problem, a groin strain, or just the way they are built. Sometimes they have been told to stretch more. Groin and hip pain in young active adults should be evaluated properly, including a physical examination for impingement signs and imaging to assess the bony morphology.
My approach is always to start conservatively. A structured physiotherapy program and activity modification can reduce symptoms meaningfully in patients with mild disease. But I am honest when the structural damage is significant enough that conservative treatment is just managing symptoms while the clock runs down on the joint.
The labrum, when it is torn cleanly and the tissue is healthy, can be repaired beautifully arthroscopically. It heals, it restores the hip’s sealing function, and the patients do well. But if someone waits two more years and the labrum degenerates beyond repair, we are now debridement rather than repair, and the long-term joint protection is much less complete.
If you are in Indore and you have hip or groin pain that has been bothering you for weeks or months, come in. A proper assessment takes less than an hour. And knowing what is happening in your hip is worth far more than hoping it resolves on its own.
10 Frequently Asked Questions About FAI Hip Impingement Treatment
1. What does hip impingement (FAI) feel like?
Most patients describe a deep ache or sharp catching pain in the groin or front of the hip. It typically worsens with deep hip bending, sitting for long periods, getting out of a low car seat, or rotating the hip inward. Some patients feel a clicking or locking sensation. The pain is usually inside the joint, not on the surface of the hip.
2. Can FAI heal on its own without treatment?
The bony abnormality that causes FAI (the cam bump or pincer rim) does not change on its own. However, symptoms can be managed conservatively for many patients. The problem is that every day the impingement continues, the labrum and cartilage take small amounts of additional damage. Conservative treatment manages symptoms but does not stop that process. Early treatment protects the joint better than prolonged waiting.
3. Do I definitely need surgery for FAI?
Not necessarily. Many patients with mild to moderate FAI can function well with physiotherapy and activity modification for years. Surgery becomes appropriate when symptoms significantly limit function, when conservative treatment has failed, or when imaging shows significant labral tearing or cartilage damage that needs direct treatment.
4. What is the difference between cam and pincer impingement?
Cam impingement is when the femoral head (ball) has a bony bump making it non-round. It is more common in men and athletes. Pincer impingement is when the socket over-covers the femoral head, crushing the labrum on deep hip bending. It is more common in women. Most patients have a combination of both, which is called mixed impingement.
5. What is a labral tear and does FAI always cause one?
The labrum is a ring of fibrocartilage around the rim of the hip socket. FAI causes it to be repeatedly pinched, which leads to tearing over time. In a study of patients diagnosed with FAI syndrome, 83% had a confirmed labral tear on MRI. It is not guaranteed from day one, but prolonged untreated FAI almost always results in labral damage.
6. How long does hip arthroscopy recovery take for FAI?
Return to normal daily activities typically takes 6 to 12 weeks. Return to sport is 4 to 6 months for non-contact activity and 6 to 9 months for full competitive sport. Recovery is longer than knee arthroscopy because labral tissue repairs need more healing time and the hip requires careful rehabilitation to avoid compensatory movement patterns.
7. Will FAI come back after surgery?
If the bony reshaping is accurate and physiotherapy is completed properly, recurrence of the bony impingement is uncommon. Re-tears of the labrum can occur if rehabilitation is rushed or if the patient returns to high-demand sport before adequate healing. The re-operation rate for hip arthroscopy is approximately 5.5%.
8. Is FAI related to hip arthritis?
Yes, directly. Cam-type FAI is well-established as a cause of early hip osteoarthritis. The repeated grinding of the aspherical femoral head against the cartilage causes progressive cartilage loss that is the foundation of arthritis. Treating FAI at the right time is, in effect, an arthritis prevention strategy for the hip.
9. What sports put you at highest risk for developing FAI?
Any sport that involves deep hip flexion, pivoting, and rotation during adolescence increases the risk of cam deformity development. Football, wrestling, kabaddi, cricket (particularly wicket-keeping), cycling, gymnastics, and martial arts have the highest associations. This is because the growth plate of the femoral head during teenage years is vulnerable to mechanical stress that may alter the final shape of the femoral head.
10. How is FAI diagnosed in Indore and what tests are needed?
Diagnosis requires a combination of a clinical history, physical examination (including the FADIR test and assessment of hip range of motion), and imaging. X-rays of the pelvis assess bony morphology and measure the alpha angle. MRI or MR arthrography is used to evaluate the labrum and cartilage in more detail. A diagnostic intra-articular injection is sometimes used to confirm that pain is coming from inside the joint. A consultation with an orthopedic specialist who is familiar with FAI is the starting point for anyone with persistent groin or hip pain in Indore.


