

Most people who come in with cervical spondylosis have already spent months confused. They have an MRI report full of words like “disc osteophyte complex,” “foraminal narrowing,” and “degenerative changes,” and nobody has sat down with them and explained what any of it actually means for their life. Some have been told to rest. Some have been sent home with a generic exercise sheet. A few have been doing stretches for months that were quietly making things worse. This article exists to fix all of that.
Cervical spondylosis is one of the most common conditions seen in orthopaedic practice, and one of the most misunderstood. NCBI data shows it is present in roughly 25% of people under 40, 50% of those above 40, and up to 85% of people over 60. Most of them have no symptoms at all. The ones who do often spend years getting incomplete explanations. That changes here.
What Is Spondylosis ?
The word spondylosis comes from the Greek word for vertebra. It describes degenerative changes in the spine, specifically the wearing down of the intervertebral discs and the joints between vertebrae. In plain language: the cushions between your neck bones are losing their height and elasticity, and the bones are responding by forming small bony growths called osteophytes or bone spurs.
This is not a disease in the way an infection is a disease. It is wear. It is what happens when a joint has been under load for years. The same process that causes osteoarthritis in a knee causes spondylosis in the spine. Your discs, which are mostly water when you are young, gradually lose hydration and become thinner and less flexible. The space between vertebrae narrows. The facet joints, which are small joints at the back of each vertebra, develop their own arthritic changes. Bone spurs form along the edges of vertebrae as the body tries to stabilize the area.
When this happens in the neck, it is called cervical spondylosis. When it happens in the lower back, it is lumbar spondylosis. Both can exist at the same time. The cervical spine, particularly the C5-C6 and C6-C7 levels, bears the most movement and load in the neck and is therefore most commonly affected.
One clarification that matters: spondylosis is different from spondylitis, spondylolysis, and spondylolisthesis, four words that cause enormous confusion. Spondylitis means inflammation of the vertebrae, as in ankylosing spondylitis, which is an autoimmune condition. Spondylolysis means a stress fracture in a specific part of the vertebra called the pars interarticularis. Spondylolisthesis means one vertebra has slipped forward over another. Spondylosis, the one this article focuses on, is degenerative joint disease of the spine. Different conditions, different management.
Why Are So Many People in Their 20s and 30s Developing Cervical Spondylosis?
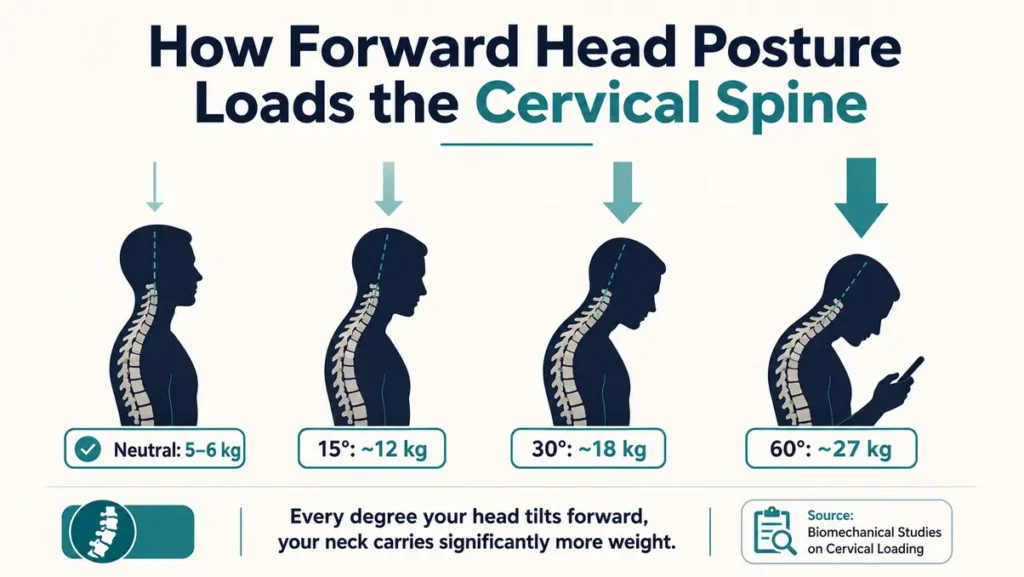
Spondylosis used to be considered a condition of aging. It still is, in the sense that degeneration increases with age. But the pattern has shifted dramatically. Young adults and even teenagers are now presenting with degenerative cervical changes that would previously have been expected decades later. The reason is posture, specifically the chronic forward head posture that comes with how people now spend their days.
Your head weighs approximately 5 to 6 kilograms in neutral position. Every inch it moves forward from that neutral position effectively increases the load on the cervical spine. Published biomechanical data consistently shows that at 60 degrees of forward flexion, which is the angle most people hold while looking at a phone, the compressive force on the cervical spine rises to the equivalent of carrying roughly 27 kilograms on your neck. The structures bearing that load are not designed for it, at least not for hours every single day, year after year.
The result is that the anterior flexor muscles of the neck weaken because they are chronically elongated and underused. The posterior muscles tighten and fatigue because they are constantly working to resist the forward pull. The discs at C5-C6 and C6-C7 experience accelerated loading and begin degenerating faster than they should. The curve of the cervical spine, which should be a gentle C-shape when viewed from the side, gradually straightens or even reverses. A straight or reversed cervical curve means the load is now distributed poorly across the discs, accelerating degeneration further.
Clinical data from PMC confirms this trend: the incidence of cervical spondylosis is increasing in young and middle-aged adults in ways that were not seen in previous generations. This is not genetic misfortune. It is a lifestyle and posture problem, and in many cases, it is reversible or at least stoppable if caught early enough.
1. Why Do My Neck Exercises Make Cervical Spondylosis Worse Instead of Better?
This is one of the most important questions in this entire article, and it does not get answered clearly enough.
The cervical spine has two important structural facts. First, the discs and vertebral bodies sit at the front of the spinal column. Second, the nerve roots exit from the back of the spine, through openings called intervertebral foramina. When you extend your neck backward, those foraminal openings narrow. When there are already bone spurs or disc bulges pressing from the front, extension compresses the nerve roots even further. That is why looking upward, tilting your head back and to the side, and certain rotation stretches can make symptoms significantly worse in someone with cervical spondylosis.
Many generic exercise guides recommend these very movements. They are appropriate for people with pure muscle tightness and no structural degeneration. In someone with confirmed disc narrowing, bone spurs, or foraminal compromise, they can inflame nerve roots and increase pain, numbness, and dizziness for days.
The correct approach works with the anatomy, not against it. Gentle neck flexion, which means bringing the chin toward the chest, actually opens the foraminal spaces and reduces nerve root compression. Chin tucks, which are controlled retraction movements that bring the head back over the shoulders without tilting up or down, are one of the most evidence-supported exercises for cervical spondylosis. Isometric strengthening exercises, which contract the neck muscles against resistance without moving the joint through full range, build strength without putting the already compromised disc spaces through painful positions.
If exercises have been making symptoms worse, the exercises are almost certainly wrong for this specific condition. This is not a reason to stop all movement. It is a reason to get the right exercises from someone who understands the anatomy.
2. Why Do Physiotherapists Recommend Stretches That Increase Pain, Numbness, or Dizziness?
The honest answer is that not all physiotherapists are equally trained in cervical spine conditions, and generic protocols are often applied where individualized assessment is needed. A stretch that is appropriate for someone with pure muscular tightness can be harmful for someone who has nerve root compression from disc and osteophyte disease.
Dizziness or increased numbness during a neck stretch is a warning signal from the nervous system, not a sign that the stretch is “working.” If a movement consistently provokes dizziness, electric sensations down the arm, or worsening numbness, that movement needs to be stopped and the clinical picture needs to be reassessed. A good physiotherapist will modify the protocol immediately. If they do not, seek a second opinion from someone with specific spine rehabilitation training.
What “Disc Bulge,” “Stenosis,” “Osteophytes,” and “Foraminal Narrowing” Actually Mean
MRI reports are written for clinicians, not patients. The language is technical and the phrasing can sound catastrophic. Here is a plain explanation of the terms most commonly found in cervical spondylosis reports.
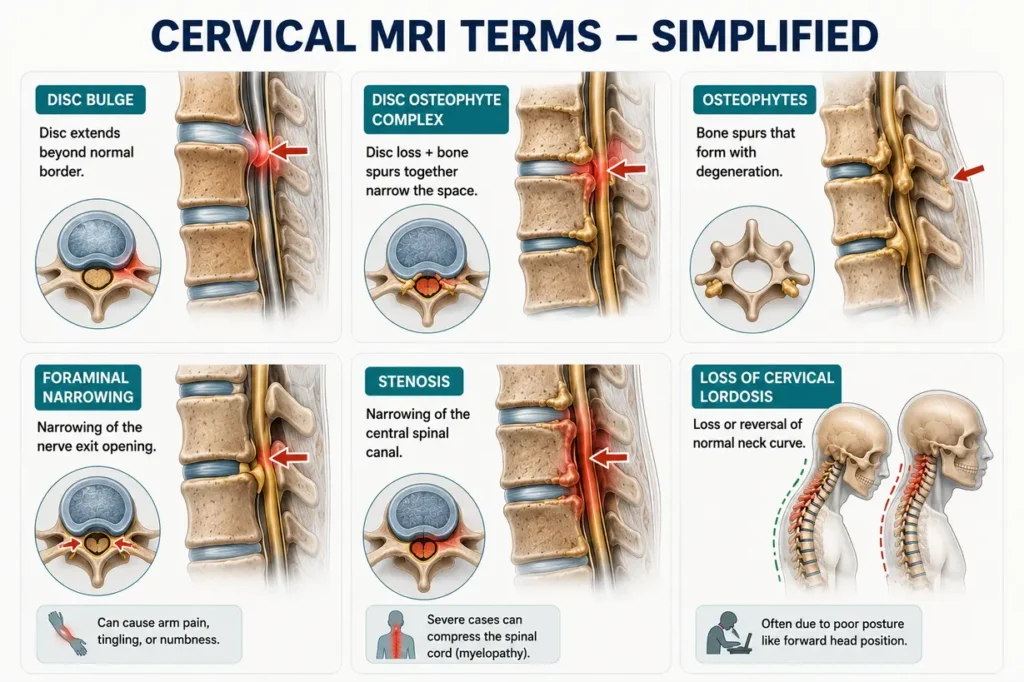
- Disc bulge: The outer fibrous ring of the disc is intact, but the disc is pressing slightly outward beyond its normal border. This is extremely common and often asymptomatic. A bulge in isolation, without nerve contact, rarely causes significant symptoms.
- Disc osteophyte complex: A combination of a disc that has lost height and bone spurs that have formed at the disc edges. Together they can narrow the space available for nerve roots.
- Osteophytes: Bone spurs. The spine forms these in response to instability and degeneration, as a way of trying to stabilize the area. They are not inherently dangerous but can press on nerve roots or, in severe cases, on the spinal cord itself.
- Foraminal narrowing: The openings through which nerve roots exit the spine are reduced in diameter. This is the finding most directly linked to arm pain, tingling, and numbness. Moderate foraminal narrowing may be asymptomatic. Severe narrowing with nerve contact produces radiculopathy.
- Stenosis: Narrowing of the central spinal canal. When severe, this can compress the spinal cord rather than individual nerve roots, a condition called myelopathy, which is more serious and may require surgical consideration.
- Loss of cervical lordosis: The normal C-shaped curve of the neck has reduced or reversed. This redistributes load poorly across the discs and is often a result of chronic forward head posture.
3. Can Cervical Spondylosis Cause Dizziness, Vertigo, or Feeling Off Balance All Day?
Yes, and this association is more common than most patients are told.
The cervical spine contains a dense network of proprioceptive receptors, nerve endings that constantly send positional information to the brain about where the head is in space. When degeneration, muscle tension, or nerve irritation disrupts this signaling, the brain receives conflicting position information from the neck, the inner ear, and the eyes. The result can be dizziness, a feeling of being off balance, light-headedness, or even true vertigo. This is called cervicogenic dizziness.
Additionally, osteophytes at higher cervical levels can, in rare cases, compress or irritate the vertebral arteries that run through the transverse processes of the cervical vertebrae. Rotation or extension movements that already provoke dizziness should be avoided until a proper clinical assessment rules out vascular involvement.
Dizziness from cervical spondylosis typically worsens after prolonged sitting at a desk or looking at a screen, improves with gentle movement and rest, and is often accompanied by neck pain or stiffness. If dizziness is sudden, severe, or associated with vision changes or difficulty speaking, it needs urgent neurological evaluation regardless of spondylosis history.
4. Why Do I Feel Tingling, Numbness, or Electric Shock Sensations in My Arms and Fingers While Sleeping?
Night-time symptoms are one of the most distressing presentations of cervical spondylosis, and they have a clear mechanical explanation.
When you sleep, certain positions, particularly on your stomach with the head rotated, or with a pillow that is too high or too thick, place the cervical spine in sustained positions of extension or lateral flexion. These positions narrow foraminal spaces for hours at a time. When nerve roots are already compromised by osteophytes or disc material, sustained positional compression at night produces tingling, numbness, and that characteristic electric shock or burning sensation that travels into the arm, forearm, and fingers.
The specific fingers affected give clinical information about which nerve root is involved. Symptoms predominantly in the thumb and index finger suggest C6 root involvement. Middle finger predominance suggests C7. Ring and little finger symptoms suggest C8. This dermatomal pattern, when matched with imaging findings, helps confirm the level of compression and guides treatment decisions.
Sleeping on your back with a cervical contour pillow that supports the natural curve of the neck without pushing the head forward, or on your side with a pillow that keeps the neck in neutral alignment with the rest of the spine, significantly reduces night-time symptoms for most patients.
5. Can Cervical Spondylosis Feel Like Anxiety, Panic Attacks, Stroke Symptoms, or a Heart Problem?
This is a question many patients are afraid to ask, and the answer is yes, it can mimic all of these in specific ways.
Nerve root irritation at the upper cervical levels, particularly C4 and C5, can produce chest tightness, shoulder pain, and a sensation that patients frequently describe as something pressing on the chest. This is referred pain, where the source of the irritation is in the neck but the symptom is felt somewhere the nerve travels to. It can feel exactly like cardiac pain and has led many patients through cardiology workups before the cervical origin is identified.
The anxiety and panic-like symptoms from cervical spondylosis often come from the autonomic nervous system. Chronic neck muscle tension, particularly in the suboccipital muscles at the base of the skull, can irritate structures that influence sympathetic nervous system tone, producing symptoms like heart palpitations, a feeling of internal trembling, sweating, and a sense of impending doom that resembles a panic attack.
The clinical clue that neck is involved is that these symptoms are consistently worse after prolonged desk work, after sleeping in a poor position, or after activities that load the cervical spine. That temporal relationship is often what guides the diagnosis. If any of these symptoms are new, severe, or accompanied by facial weakness, speech changes, or loss of arm or leg function, they need emergency evaluation first to rule out stroke or other neurological events.
6. Why Do Headaches Start from the Neck and Travel to the Forehead or Eyes?
These are cervicogenic headaches, and they are among the most underdiagnosed conditions in primary care.
The upper cervical nerve roots, particularly C1, C2, and C3, share referral pathways with the trigeminal nerve, which is the main sensory nerve of the face. This neurological overlap, called the trigeminocervical complex, means that pain from the upper neck can be felt in the forehead, around the eyes, at the temples, or across the top of the skull.
Patients with cervicogenic headaches typically notice that the headache starts at the base of the skull or in the upper neck, and then spreads forward. Pressing on the suboccipital muscles at the base of the skull reproduces or intensifies the headache. The headache is consistently worse after desk work, driving, or sleeping in a poor position. It does not throb like a migraine, though it can be accompanied by nausea and light sensitivity, which causes frequent misdiagnosis as migraine.
Tightness in the suboccipital muscles from forward head posture and chronic cervical loading is one of the most common triggers. Addressing the cervical spine mechanically, through posture correction, targeted muscle release, and chin tuck exercises, often reduces headache frequency significantly without medication.
7. Can Bad Posture and Phone Use Permanently Damage the Cervical Spine?
Permanent is a strong word, but the honest answer is: sustained poor posture over years causes structural changes that cannot be fully reversed.
The loss of cervical lordosis, the straightening of the natural neck curve, can become a fixed structural change if postural habits are not corrected. Disc degeneration, once it has progressed beyond mild thinning, does not regenerate. Bone spurs that have formed do not disappear on their own. Foraminal narrowing from chronic degeneration is a structural reality.
What can change is the trajectory. Caught early, the process can be significantly slowed. Muscle strength can be restored. Posture can be corrected enough to reduce daily load on compromised discs. Inflammation can be managed. Symptoms can be reduced substantially even when structural changes exist.
The specific postures that accelerate damage: looking down at a phone for more than 20 to 30 minutes at a time without breaks, working on a laptop screen positioned below eye level, sleeping prone (on the stomach), and sitting in chairs without lumbar support that causes the thoracic spine to round and the head to compensate by moving forward.
8. Why Does Neck Pain Become Worse After Working on a Laptop or Mobile Phone?
Because the position most people adopt while using screens is precisely the worst possible position for the cervical spine.
When a laptop is placed on a desk without a stand, the screen is below eye level. The user drops the chin and flexes the neck forward to look at it. This position, held for hours, does three things simultaneously: it places the discs under compressive load, it stretches and fatigues the posterior neck muscles, and it reduces blood supply to the paraspinal muscles through sustained contraction. The result is disc irritation, muscle fatigue, spasm, and the familiar dull ache that builds through a working day and peaks in the evening.
Screen position matters more than most people realize. The top third of the screen should be at eye level. The screen should be directly in front, not offset to one side. Phone use should involve raising the phone to eye level rather than dropping the head. These are small changes that meaningfully reduce the daily load on the cervical spine.
9. Why Do MRI Reports Sound Terrifying But Doctors Still Say “Nothing Serious”?
Because MRI reports describe anatomy, not symptoms. And the correlation between what an MRI shows and what a patient actually experiences is weaker than most people assume.
Studies consistently show that a significant proportion of people with severe-looking MRI changes have no symptoms at all, while some patients with modest imaging findings have significant pain and disability. The MRI tells you what the structure looks like. It does not tell you how irritated the nerve is, how inflamed the surrounding tissue is, or how the patient is actually functioning. That clinical picture requires examination, not imaging alone.
When a doctor says “nothing serious,” they typically mean: there is no spinal cord compression, no instability, no tumor, no infection, and no finding that requires urgent surgical consideration. The degeneration visible on the MRI is real, and it explains the symptoms, but it does not require surgery. This reassurance is medically accurate. The disconnect happens because patients hear “nothing serious” and assume their pain is imaginary or being dismissed. It is neither. The pain is real. The degeneration is real. The management is just conservative rather than surgical.
How to Know If a Nerve in Your Neck Is Being Compressed
Nerve root compression, called cervical radiculopathy, produces a specific pattern of symptoms that follows the nerve’s distribution rather than staying in the neck itself.
The key features of nerve root compression are: pain, tingling, or numbness that travels from the neck into the shoulder, arm, forearm, or hand in a specific pattern; weakness in specific muscle groups supplied by that nerve root; and reflexes that may be reduced or absent at specific levels. Pure neck pain without any arm component is usually muscular or discogenic rather than true nerve root compression.
A clinical provocation test called Spurling’s test, where the examiner extends the neck and tilts it toward the symptomatic side while applying gentle downward pressure, reproduces radicular symptoms when a nerve root is significantly compressed. The test should be performed by a clinician, not attempted at home. Positive Spurling’s combined with matching dermatomal symptoms and MRI findings at the corresponding level provides high diagnostic confidence.
10. What Exercises Are Safe and What Exercises Make Cervical Spondylosis Worse
This section addresses the most common exercise-related harm that reaches the clinic, which is people continuing movements that their spine is telling them to stop.
Exercises that are generally safe and beneficial in cervical spondylosis:
- Chin tucks: controlled retraction of the head straight back without tilting up or down, strengthening the deep cervical flexors and correcting forward head posture
- Isometric strengthening: pressing the head gently against the hand in forward, backward, and lateral directions without movement, held for 5 seconds and released
- Shoulder blade retraction: pulling the shoulder blades together and down, reducing the forward rounding that contributes to forward head posture
- Gentle cervical flexion: slowly bringing the chin toward the chest, which opens the foraminal spaces posteriorly
- Levator scapulae stretch with shoulder anchor: sitting and gripping the chair with the hand on the affected side, then gently tilting the head away and slightly forward, stretching the muscle without compressing posterior structures
Movements to avoid with confirmed cervical spondylosis:
- Full cervical extension (looking straight up): narrows foraminal spaces and compresses posterior structures
- Extension combined with rotation (looking up and to one side): the position of maximum foraminal compromise
- Aggressive cervical traction without clinical guidance
- Heavy overhead lifting without cervical stabilization
- Prone-lying exercises that require sustained neck extension
11. How Do I Know If a Nerve in My Neck Is Being Compressed?
The clearest signal is symptoms that travel away from the neck. Pure neck pain stays in the neck. Nerve root involvement produces a radiating pattern into the shoulder, arm, forearm, or hand. Burning, electric, or shooting quality to the pain, particularly if it follows a clear dermatomal pathway, suggests nerve involvement. Weakness in grip strength, difficulty with fine motor tasks in the hand, or a feeling that the arm is heavy or unreliable are signs of more significant compression that need clinical evaluation promptly.
12. Why Do Symptoms Become Worse at Night or After Waking Up?
Two mechanisms operate here. The first is positional: sleeping positions that sustain the neck in extension, lateral flexion, or rotation for hours compress already narrowed foraminal spaces and produce symptoms that peak in the early morning. The second is inflammatory: disc and joint inflammation follows a circadian pattern similar to other arthritic conditions, with stiffness and pain often highest in the morning before the joints have been mobilized and warmed up.
The morning stiffness of cervical spondylosis typically loosens within 30 to 60 minutes of gentle movement. If morning stiffness lasts longer than 90 minutes and is accompanied by significant systemic symptoms like fatigue or eye inflammation, inflammatory spondylitis rather than degenerative spondylosis needs to be considered.
Treatment for Cervical Spondylosis in Indore: What Actually Works
The treatment landscape for cervical spondylosis is well-established, and the vast majority of patients do not need surgery. The goal of treatment is to reduce inflammation, restore function, correct the mechanical loading patterns that are accelerating degeneration, and protect the nerve roots from further irritation.
Conservative management, which resolves symptoms in roughly 80 to 90 percent of patients, includes:
Structured physiotherapy with a cervical-specific protocol rather than a generic one. This means chin tuck retraining, isometric strengthening, postural correction, and manual therapy targeted to the affected segments. The physiotherapist needs to understand which movements to avoid as clearly as which movements to prescribe.
Anti-inflammatory medication in the acute phase to reduce disc and nerve root inflammation. NSAIDs are the first-line pharmacological choice. Muscle relaxants may be added if significant spasm is present. Neither is a long-term solution without addressing the mechanical cause.
Cervical traction, when applied correctly by a trained clinician, gently separates the disc spaces and reduces nerve root compression. It is particularly useful for radiculopathy. Self-applied traction devices without clinical guidance carry risk and should be avoided.
Epidural steroid injections targeted to the affected nerve root level can provide significant short-term relief in patients with severe radiculopathy who have not responded to conservative measures. They are a bridge to rehabilitation, not a standalone treatment.
At Dr. Prince Uchadiya Orthopaedic And Joint Care Clinic in Indore, patients with cervical spondylosis undergo clinical examination, review of imaging, and a structured management plan that addresses both the symptomatic relief and the underlying mechanical factors. The orthopaedic specialist consultation forms the starting point for a protocol-based approach rather than a generic prescription.
13. Can Cervical Spondylosis Affect Eyesight, Cause Blurry Vision, Burning Eyes, or Eye Pressure?
Yes, though the pathways are indirect and less commonly discussed.
Compression or irritation of the upper cervical nerve roots and the suboccipital muscles that attach at the base of the skull can influence the sympathetic nerve supply to the eye, producing sensations of eye pressure, burning, or blurring. The greater occipital nerve, which emerges at C2, has referral patterns that reach the eye socket and forehead. Patients with upper cervical spondylosis sometimes describe a sensation of pressure behind the eye or visual blurring that correlates with neck pain episodes and resolves when neck symptoms improve.
This is not the same as vision problems from a direct neurological cause, and any new or progressive vision change needs ophthalmological evaluation before it is attributed to the cervical spine. But for patients who have already been cleared ophthalmologically and continue to experience intermittent eye pressure or blurring alongside cervical symptoms, the neck is a legitimate contributing factor.
14. Why Do Some People Remain in Pain Even After Surgery or Spinal Fusion?
This is called failed back (or failed neck) surgery syndrome, and it happens for several reasons.
Surgery for cervical spondylosis addresses the structural problem at a specific level, either by removing a disc and fusing the vertebrae (ACDF) or by decompressing the spinal canal from behind (laminoplasty or laminectomy). When the correct level is treated, and the nerve root or spinal cord decompression is successful, most patients improve significantly. When post-surgical pain persists, the most common reasons are: the treated level was not the primary pain generator and the actual source was at a different level; adjacent level degeneration has accelerated because the fused segment transfers load to neighboring discs; the nerve root had been compressed so long that permanent fiber damage occurred before surgery; or muscular and postural patterns that caused the original problem were never corrected and continue to load the spine.
This is why surgery for cervical spondylosis is the last resort rather than an early option, and why non-surgical management including posture correction and rehabilitation is almost always tried first. Current NCBI guidelines support surgical consideration primarily for myelopathy (spinal cord compression) and severe radiculopathy unresponsive to 6 to 12 weeks of conservative management.
15. Can Cervical Spondylosis Be Reversed Naturally Without Surgery?
Structural reversal of established degeneration is not possible. Discs that have lost height do not regain it. Bone spurs that have formed do not dissolve. This is the reality of degenerative change.
What is possible, and what many patients achieve, is functional reversal: symptoms resolve, nerve root irritation settles, strength and mobility return, and quality of life returns to normal. This happens through a combination of anti-inflammatory management, mechanical load reduction through posture correction, targeted strengthening of the supporting musculature, and modification of the daily habits that were accelerating degeneration.
Whether symptoms return depends on whether the mechanical causes are addressed. A patient who corrects their workstation setup, learns chin tuck exercises, and maintains their cervical strengthening program has a fundamentally different trajectory from one who takes anti-inflammatories for six weeks and then returns to exactly the same patterns that caused the problem. The spine responds to how it is loaded. Change the loading, and you change the symptoms.
16. Why Do So Many People Say They Were Doing the “Wrong Stretches” for Years?
Because the most widely circulated neck exercise advice is generic and does not account for the anatomy of spondylosis.
Stretches like cervical circles (rotating the head all the way through a full circle), looking up toward the ceiling, tilting the head back to the side, and hanging the head forward in full flexion are commonly taught and frequently harmful in the context of structural disc and joint disease. They feel like they are “releasing” something. In some cases they are, temporarily reducing muscular tension. But in doing so they are also compressing nerve roots, loading compromised facet joints, and in the case of full cervical extension, potentially stressing the vertebral arteries.
The distinction between safe and unsafe cervical exercise requires understanding whether the primary problem is muscular, discogenic, or involving nerve roots. Without that clinical distinction, a standard exercise sheet applied to everyone produces the outcome that so many patients describe: months of effort with worsening symptoms, followed by the frustrating discovery that the approach was wrong from the start.
17. Can Poor Sleeping Posture or the Wrong Pillow Silently Worsen Cervical Degeneration?
Yes. Sleep accounts for 7 to 9 hours of positional loading every day. Over years, that is an enormous cumulative load on the cervical spine.
Pillows that are too high push the head into lateral flexion when sleeping on the side and into cervical flexion when sleeping on the back. Pillows that are too flat allow the head to drop in side-lying, creating the opposite lateral flexion. Stomach sleeping, for any reason, requires the head to be rotated to one side for hours, which combines rotation and extension and is the worst possible sleeping position for someone with cervical spondylosis or radiculopathy.
The correct pillow for cervical spondylosis depends on the individual’s shoulder width and primary sleeping position. A cervical contour pillow, which has a raised section to support the natural neck curve when supine and a higher section to fill the shoulder gap in side-lying, is generally better than a standard pillow. Pillow selection is rarely discussed in clinical consultations but has a measurable impact on morning symptom severity.
18. Why Do Doctors Ignore Neck Pain in Younger People or Dismiss It as Stress and Anxiety?
This is a legitimate frustration, and it reflects a genuine clinical bias.
Cervical spondylosis has historically been considered a condition of aging. A 25-year-old or 30-year-old presenting with neck pain, arm tingling, and headaches is more likely to be evaluated for stress, anxiety, or tension headaches than for structural cervical degeneration. The workup is different. Stress and anxiety are more common in that demographic. And MRI for a young adult with neck pain is not the first clinical step in most healthcare systems.
The problem is that prolonged forward head posture from screen use is creating genuine structural changes in younger people, changes that then go unidentified for years while the degeneration progresses. If symptoms are consistent, if they follow a mechanical pattern (worse with sustained screen use, better with rest, worse in certain positions), if arm tingling follows a dermatomal pattern, and if postural abnormalities are visible on examination, imaging is warranted regardless of age.
Persistent, mechanical neck pain in a younger person that does not respond to rest and simple analgesia within 4 to 6 weeks deserves clinical evaluation from an orthopaedic or spine specialist. If you are in Indore and this describes your situation, a structured second opinion that includes examination and appropriate imaging can clarify the picture quickly.
19. Why Do So Many Patients Say “I Wish Someone Explained This Earlier”?
Because the information gap between what patients are told and what they need to understand is significant, and it has real consequences.
A patient who understands what foraminal narrowing means will not perform the very movements that compress that foramen. A patient who understands why the neck curve matters will change their workstation setup. A patient who understands the difference between pain from muscle and pain from nerve compression will not push through warning signals that they should be stopping for. A patient who understands that spondylosis is mechanical, not a sentence, will engage with rehabilitation rather than waiting for it to magically improve.
Education is part of treatment for cervical spondylosis. It changes what patients do between appointments, and what patients do every day matters far more than what happens in a clinic twice a week. This article is an attempt to give people what they should have been told at the beginning.
At Dr. Prince Uchadiya’s Clinic in Indore, the consultation for cervical spondylosis includes an explanation of findings, the mechanical rationale behind each treatment recommendation, and specific guidance on exercises and posture. Patients leave understanding their condition, not just their prescription. For back pain and spine-related concerns, the back pain specialist clinic in Indore provides both diagnosis and structured management under the same roof.
Cervical spondylosis is common, it is manageable, and in most people it does not lead to surgery. Understanding it accurately is the first step to managing it correctly. The second step is working with someone who can translate that understanding into a plan that actually fits your spine, your life, and your daily habits.


