
Every question on this page came from a real person. Not a textbook. Not a clinical guideline. These are the exact questions patients search for at midnight after years of incomplete answers, the things they were afraid to ask, the doubts that kept them from trusting their diagnosis, and the frustrations they shared in comment sections because nobody in a clinic had taken the time to explain properly.
For a complete clinical explanation of cervical spondylosis including anatomy, exercises, MRI terminology, and treatment, read the full cervical spondylosis guide alongside this page.
Section 1: Symptoms That Confuse and Frighten People
1. Can cervical spondylosis actually cause dizziness, vertigo, or feeling off balance all day or is that something else?
Yes, and this connection is underdiagnosed. The cervical spine contains dense proprioceptive receptors that constantly send the brain information about where your head is in space. When degeneration, nerve irritation, or muscle tension disrupts that signaling, the brain receives conflicting positional data from the neck, the inner ear, and the eyes simultaneously. The result is cervicogenic dizziness: a persistent feeling of being slightly off balance, light-headed, or foggy that is worse after desk work or screen use and often accompanied by neck stiffness. This is different from inner ear dizziness. The distinction matters because the treatment is completely different. If dizziness is your main complaint alongside neck symptoms, that cervical connection needs to be assessed clinically before any other cause is assumed.
2. Can cervical spondylosis feel like a panic attack, anxiety, heart problem, or even a stroke?
Yes to all four, and this is one of the most distressing patterns I see in practice. Nerve root irritation at upper cervical levels, particularly C4 and C5, produces referred chest tightness and shoulder pain that is genuinely indistinguishable from cardiac symptoms by the patient experiencing it. Irritation of the suboccipital muscles and upper cervical structures affects the sympathetic nervous system and produces palpitations, internal trembling, sweating, and a sense of impending doom that mimics panic attacks. And significant cord compression at the cervical level can produce weakness, coordination problems, and symptoms patients describe as stroke-like. The clinical clue that neck is involved: symptoms consistently follow a pattern related to neck position and screen use. New, severe, or sudden symptoms of any of these types need medical evaluation first to rule out cardiac or neurological emergencies, always.
3. Why do I feel tingling, numbness, or electric shock sensations in my arms and fingers, especially at night?
The nerve roots that supply your arms exit the cervical spine through narrow openings called foramina. When disc degeneration and bone spurs have already narrowed those openings, sleeping in a position that adds further compression, particularly stomach sleeping or using a pillow that is too thick, compresses those nerve roots for hours. The result is tingling, numbness, burning, or electric sensations that travel into the arm, forearm, and specific fingers. Which fingers are affected tells you which nerve root is involved. Thumb and index finger symptoms point to C6. Middle finger to C7. Ring and little finger to C8. This is not random. The pattern is clinically useful and should be part of any assessment of your symptoms.
4. Why do headaches start at the base of my skull and travel to my forehead, temples, or eyes?
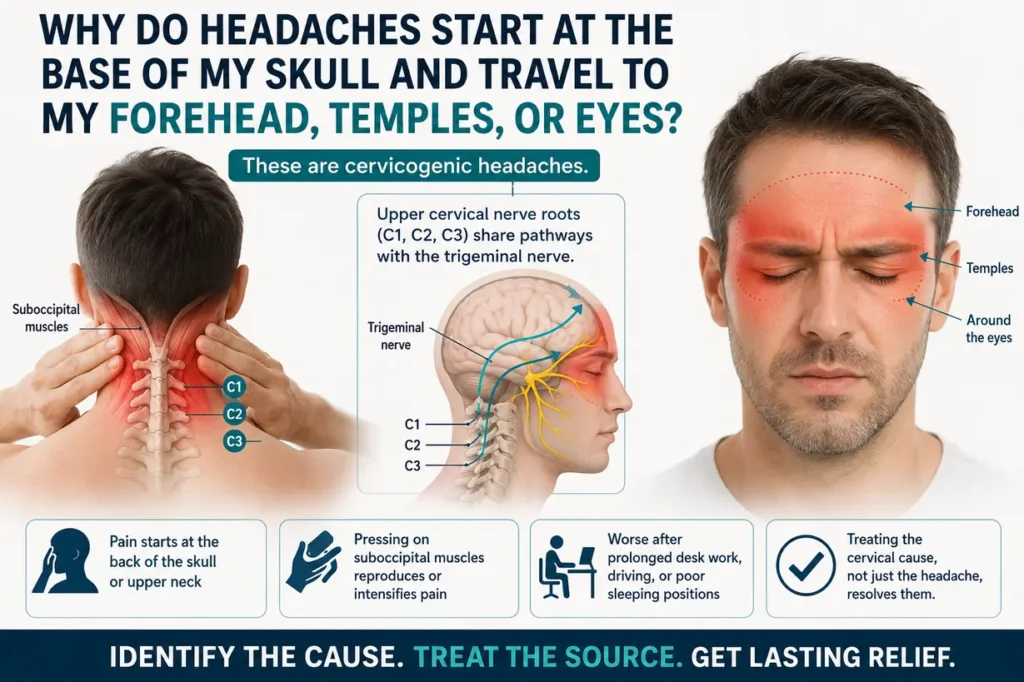
These are cervicogenic headaches, and they are frequently misdiagnosed as migraines or tension headaches. The upper cervical nerve roots, particularly C1, C2, and C3, share neurological referral pathways with the trigeminal nerve, the main sensory nerve of the face. This means pain originating in the upper cervical spine gets felt in the forehead, around the eyes, at the temples, and even behind the eyes. The distinguishing feature is that the headache starts at the back of the skull or upper neck before spreading forward, and pressing on the suboccipital muscles at the skull base reproduces or intensifies it. These headaches are consistently worse after prolonged desk work, driving, or poor sleeping positions. Treating the cervical cause, not just the headache, is what resolves them.
5. Can cervical spondylosis cause blurry vision, burning eyes, or a feeling of pressure behind the eyes?
Yes, through two indirect pathways. The upper cervical nerve roots, particularly at C2, have referral patterns that reach the eye socket and forehead. Compression or sustained irritation here can produce a sensation of eye pressure, burning, or intermittent blurring that correlates with neck pain episodes. Additionally, suboccipital muscle tension from chronic forward head posture influences the sympathetic nerve supply to the eye. Patients who have already been cleared by an ophthalmologist and continue to have intermittent eye symptoms alongside neck problems are very likely experiencing a cervical contribution. Any new or progressive vision change needs ophthalmological evaluation first.
6. Can cervical spondylosis cause ear ringing, tinnitus, or muffled hearing?
This is a less commonly discussed but genuine association. The upper cervical spine shares anatomical proximity with structures that influence the ear and its nerve supply. Chronic tension in the sternocleidomastoid and suboccipital muscles, which is common with forward head posture and cervical degeneration, can irritate the auriculotemporal nerve and affect the Eustachian tube’s function. Patients report intermittent tinnitus, a feeling of ear fullness, or mild muffled hearing that worsens during neck pain episodes and improves when the neck settles. This should be evaluated clinically, but the cervical connection is real and worth investigating when ear symptoms coexist with neck problems.
7. Why does my tongue feel numb or tingly when my neck hurts?
This is an unusual symptom that understandably frightens people, and it comes from the upper cervical nerve roots and their relationship to cranial nerve territories. C1, C2, and C3 have connections to the hypoglossal nerve, which supplies the tongue, and to the glossopharyngeal nerve. Irritation at these upper levels can produce tingling or altered sensation in the tongue, the roof of the mouth, or the throat. It is also occasionally associated with significant vertebral artery irritation from upper cervical degeneration. Tongue tingling alongside neck pain should always be clinically assessed to confirm the cervical origin and rule out neurological causes.
8. Can cervical problems affect balance and walking? I feel unsteady on my feet.
When the cervical spinal canal is narrowed enough to compress the spinal cord rather than individual nerve roots, the condition is called cervical myelopathy. This is a serious development. The spinal cord carries motor signals down to the legs, and cord compression at the neck level can produce gait disturbance, a broad-based or shuffling walking pattern, weakness in the legs, and poor balance. If you are experiencing unsteadiness on your feet alongside neck symptoms, this is not something to wait out. It needs urgent orthopaedic assessment and MRI of the cervical spine. Cervical myelopathy, if caught early and treated appropriately, can be stabilized. Left untreated, it worsens.
9. Why do symptoms sometimes improve in the morning but steadily worsen through the day?
This pattern is typical of a mechanical and postural contribution rather than a purely inflammatory one. In the morning, the spine has rested and inflammatory mediators are at lower levels. As the day progresses, sustained postures at a desk, looking at screens, sitting in chairs without proper support, and the accumulated effect of hours of forward head load inflame the already sensitized disc and nerve root structures. By evening, the load has been sustained long enough that symptoms peak. Understanding this pattern is useful because it tells you exactly where to intervene: the sustained postures of your working day. Changing those postures, building in movement breaks every 30 to 40 minutes, and addressing screen height will shift this trajectory.
10. Why does one side hurt more than the other?
Nerve roots exit the spine on both sides, but degeneration and osteophyte formation are rarely perfectly symmetrical. A disc that has collapsed slightly more on one side, or a bone spur that has grown toward one foraminal opening more than the other, will compress the nerve root on that side specifically. The result is unilateral symptoms: pain, tingling, or weakness that is predominantly on one side of the neck, shoulder, arm, or hand. The dominant arm and the most mechanically loaded side of the neck tend to develop asymmetric degeneration more often. Unilateral symptoms that clearly follow a dermatomal pattern are actually diagnostically useful because they help identify which nerve root level is involved.
11. Can cervical spondylosis cause chest tightness or difficulty breathing?
Chest tightness from cervical spondylosis is a referred symptom from C4 and C5 nerve root irritation, which supplies the diaphragm and has referral patterns into the chest wall. It does not typically cause actual breathing difficulty in the same way a lung or cardiac condition does, but the subjective sensation of tightness or pressure in the chest can be alarming. This symptom should always be evaluated to rule out cardiac and pulmonary causes first. Once those are excluded, the cervical connection can be assessed. If chest tightness consistently follows neck pain episodes and worsens with cervical loading, the spine is the likely source.
12. Can cervical spondylosis cause facial pain, jaw pain, or TMJ-like symptoms?
Yes. The trigeminal nerve, which supplies sensation to the entire face and jaw, shares referral pathways with the upper cervical nerve roots through the trigeminocervical complex. Irritation at C1, C2, and C3 can produce facial pain, jaw ache, and symptoms that closely resemble temporomandibular joint dysfunction. Patients who have been treated for TMJ without lasting improvement and also have neck problems deserve a cervical spine evaluation as part of the picture. The cervical contribution is often missed because the facial symptoms divert attention away from the neck.
13. Why do I get electric shock sensations shooting down my spine when I bend my neck forward?
This is called Lhermitte’s sign, and it is produced when flexing the neck stretches the already compressed spinal cord. The electrical sensation typically travels down the spine and sometimes into the arms or legs. It is a significant clinical finding, not a minor curiosity. Lhermitte’s sign indicates spinal cord involvement rather than just nerve root compression, and it warrants urgent MRI of the cervical spine. This is not something to manage with physiotherapy alone. It needs orthopaedic or neurosurgical assessment to determine whether cord compression is present and whether intervention is required.
Section 2: The Exercise Crisis – Why People Keep Getting Worse
14. Which neck exercises secretly make cervical spondylosis worse?
The most commonly harmful ones are cervical circles (rotating the head all the way through a full 360-degree arc), looking straight up at the ceiling, tilting the head back and to the side simultaneously, and hanging the head fully forward with no support. All of these feel like they are releasing tension, and they may briefly reduce muscular tightness. But in a spine with existing disc narrowing and osteophytes, these movements either compress nerve roots (extension and extension-rotation) or apply excessive stretch to already compromised disc structures (full unsupported flexion). The problem is that these exercises are widely taught in generic protocols that do not distinguish between muscular neck pain and structural cervical degeneration. They are not wrong for everyone. They are wrong for this specific condition.
15. Why do physiotherapy stretches sometimes increase my pain, numbness, or dizziness?
Because the stretches were designed for a different problem. A stretch that is appropriate for pure muscular tightness in someone without structural changes can load a compromised nerve root when osteophytes or disc material are already pressing on it. When a movement consistently provokes dizziness, increases arm tingling, or sends electric sensations into the limb, that movement is irritating the nervous system, not helping it. The physiotherapist needs to know this and modify the protocol. If they tell you the pain is normal and will improve with continued repetition, and it does not improve within a few sessions, that protocol is not right for your specific anatomy. Seek reassessment.
16. Can chin tuck exercises really help, or is that also something that can go wrong?
Chin tucks are among the most evidence-supported exercises for cervical spondylosis specifically, and I teach them to almost every patient I see with this condition. The movement retracts the head straight back over the shoulders, strengthens the deep cervical flexor muscles that have been chronically lengthened and weakened by forward head posture, and improves the cervical curve. The key is performing them correctly: the chin moves straight back, not upward or downward. There should be no pain, dizziness, or arm symptoms during the movement. If there are, the technique needs correction or the exercise needs to be modified based on your specific findings. Done correctly, chin tucks are one of the safest and most effective tools for this condition.
17. Are isometric neck exercises safe for someone with nerve compression?
Isometric exercises, where you press the head gently against your hand or a fixed resistance without moving the joint through range, are specifically safer than dynamic stretching for cervical spondylosis with nerve root involvement. They build muscle strength without putting the compromised disc spaces and foraminal openings through positions that could worsen compression. They should not produce pain, dizziness, or arm symptoms. If they do, the resistance is too much and needs to be reduced. When performed correctly, isometrics in forward, backward, and lateral directions are a core component of cervical rehabilitation for structural degeneration.
18. Should I stop all neck exercises during a flare-up?
During a significant flare-up with acute nerve root irritation, sharp radicular pain, or new neurological symptoms like worsening weakness, complete rest from neck exercises for a few days is reasonable. Ice applied for 15 to 20 minutes several times a day reduces acute inflammation. Anti-inflammatory medication under medical guidance helps. But complete prolonged rest from all movement is not the answer. Gentle chin tucks and maintaining reasonable activity within a pain-free range are beneficial even during flare-ups. The goal is to avoid the movements that provoke symptoms, not to become completely still, which leads to further muscle deconditioning and stiffening.
19. Can yoga worsen cervical spondylosis?
Some yoga poses can, and patients with confirmed cervical degeneration need to be specific about which poses to modify or avoid. Poses that involve significant cervical extension (Cobra, Upward Dog), full neck rotation in weight-bearing positions (some twists), or positions that load the cervical spine in flexion under body weight (Plow, Shoulder Stand, Halasana) are problematic. Gentle yoga that maintains a neutral spine, avoids extremes of cervical range, and emphasizes core and thoracic mobility is generally safe and beneficial. Tell your yoga instructor about your cervical findings so modifications can be made. A blanket “yoga is good for the spine” approach without these modifications can cause real harm.
20. Can gym training or lifting weights worsen cervical spondylosis?
Specific gym exercises carry genuine risk. Overhead pressing with heavy loads, barbell shrugs, behind-the-neck lat pulldowns, and any exercise that compresses the cervical spine axially under significant load should be avoided or significantly modified. Exercises that require sustained forward head posture, like bench press without neck support or certain rowing variations, also accumulate load on compromised disc spaces. Core strengthening, lower limb training, and upper body exercises that can be performed with the neck in neutral position are safe for most patients. The gym itself is not the enemy. Certain specific exercises are, and identifying them requires someone who understands your imaging and your anatomy.
21. Does running or intense cardio flare cervical spondylosis symptoms?
Running with significant forward head posture, which is common in people who have chronically shortened anterior neck muscles, adds repetitive compressive load to the cervical spine with each stride. Some patients notice increased neck pain, arm tingling, or headaches during or after running. The issue is not the running itself, it is the neck position during running. Cues to maintain a neutral chin position, look at the horizon rather than the ground, and relax the shoulders during running can meaningfully reduce this. If symptoms consistently worsen with running regardless of posture correction, a temporary reduction in high-impact activity while the inflammation settles is appropriate.
22. How do I know if an exercise is helping or hurting my neck?
The rules are straightforward. An exercise that is appropriate will produce no increase in arm symptoms, no dizziness, and no sharp or shooting pain during or immediately after. Mild local neck muscle fatigue after strengthening exercises is normal. Pain that persists for more than a few hours after an exercise session, any new or increased arm tingling or numbness, or dizziness provoked by the movement are signals to stop that specific exercise and report back to your clinician. Pain that is still elevated the following morning compared to your baseline before the exercise is a clear signal the exercise is wrong for your current stage. Do not push through warning signals from the nervous system.
Section 3: Technology, Lifestyle, and the Modern Neck
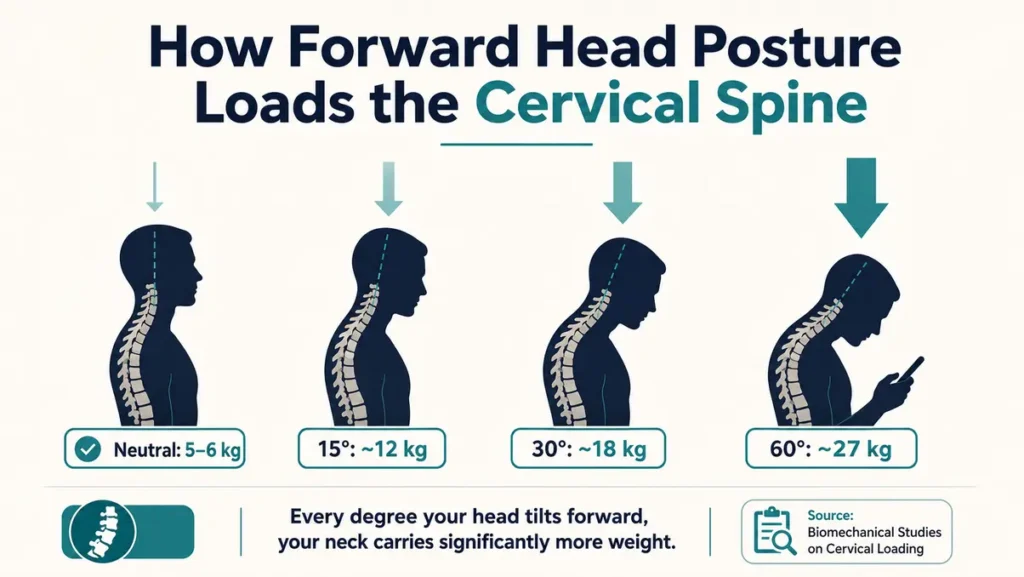
23. Is phone use causing an epidemic of cervical spondylosis? What is “tech neck”?
“Tech neck” is the informal term for the cervical degeneration driven by chronic forward head posture from screen use, and yes, it is a genuine epidemic. The problem is not phones and screens themselves. The problem is the sustained position most people adopt while using them. Looking down at a phone held in the lap places the cervical spine in 60 degrees of forward flexion for hours. Biomechanical data shows that at 60 degrees, the effective load on the cervical spine rises to the equivalent of approximately 27 kilograms. The structures are not designed to sustain that load for hours every day, year after year. The result is accelerated disc degeneration and premature loss of the cervical curve in people who would not otherwise experience these changes for decades. The intervention is not giving up screens. It is learning to hold them at eye level and taking regular breaks.
24. Why are teenagers and people in their 20s and 30s suddenly developing cervical degeneration?
Because they have had screens at eye level or below since childhood, and many of them have spent thousands of hours in sustained forward head posture by the time they are 20. The cervical discs begin responding to abnormal load early in life. By the late teens and early 20s, some patients already show loss of cervical lordosis and early disc changes on MRI that would have been considered unusual in someone under 40 two generations ago. This is not genetic inevitability. It is a load management failure accumulated over years. Caught at this stage, the trajectory can be changed. Left unaddressed, the degeneration continues to progress.
25. Which professions carry the highest risk of cervical spondylosis?
The common factor across high-risk professions is sustained forward head posture or repetitive cervical loading. Hairdressers and beauticians work with their heads tilted forward and down for hours. IT professionals and software developers spend the working day with screens below eye level. Surgeons, particularly those doing fine operative work while leaning forward. Dentists. Nurses who work with patients in bed. Artists and illustrators who work on horizontal surfaces. Drivers who sit without adequate head support. Cashiers, data entry workers, and anyone whose primary working position places the head forward of the shoulders for sustained periods. The injury is cumulative, not acute. The risk is not the task itself but the position held while doing it, repeated over years.
26. How many hours of screen time per day actually damages the neck?
There is no single threshold that applies to everyone because the damage depends on screen position, not screen duration alone. A screen at eye level used for 8 hours causes far less cervical loading than a screen positioned below eye level used for 3 hours. The practical guidance: position your screen so that your eyes meet the top third of it without dropping your chin. Take a deliberate posture break every 30 to 40 minutes, stand up, reset your head position, do five chin tucks. Phone use specifically should involve raising the phone to eye level rather than dropping the head. These changes, implemented consistently, substantially reduce daily cervical load regardless of total screen time.
27. Can studying for long hours damage the cervical spine in students?
Yes, and this is one of the most under-discussed risk factors in younger patients. Students spend hours reading textbooks placed flat on a desk, writing notes with the head dropped forward, and working on laptops or tablets without appropriate stands. The academic environment essentially requires sustained forward head posture, and school and college desks are rarely designed with cervical ergonomics in mind. Students who spend 6 to 10 hours a day in this position through school and then university years are accumulating significant cumulative cervical load through their formative years. Simple interventions, a book stand, a laptop stand, a reminder to do chin tucks every hour, make a real difference at this stage before structural changes have established themselves.
28. Does working from home worsen cervical degeneration compared to an office?
Often yes, because home setups rarely have the ergonomic infrastructure of a properly set-up office. People work from kitchen tables, sofas, and beds with laptops that are not elevated. The boundary between work and rest disappears, meaning longer hours in compromised positions without the movement breaks that office environments naturally provide. Investing in a monitor stand, an external keyboard, and an adjustable chair with lumbar support transforms a home workspace from a cervical risk factor into a neutral one. This is not a luxury for people with cervical spondylosis. It is part of treatment.
Section 4: Sleep, Pillows, and Night Symptoms
29. Can sleeping posture silently worsen cervical degeneration over years?
Sleep accounts for 7 to 9 hours of positional loading every day. Over years, that is a significant cumulative force on the cervical spine. Stomach sleeping is the worst position for anyone with cervical degeneration because it requires the head to be fully rotated to one side for hours, combining rotation and extension simultaneously. Sleeping with a pillow that is too high creates sustained lateral flexion in side-lying and excessive cervical flexion when supine. Sleeping with a pillow that is too flat drops the head in side-lying and does the opposite. The correct pillow height for cervical spondylosis supports the natural curve of the neck in back-sleeping and fills the shoulder-to-ear distance in side-sleeping without pushing the head forward. This sounds like a small detail. In practice, correct pillow choice is one of the most impactful changes patients make for their morning symptoms.
30. Which sleeping positions are safest and which are most harmful for cervical spondylosis?
Back sleeping with a cervical contour pillow that supports the natural neck curve is generally the safest. Side sleeping with a pillow thick enough to keep the neck parallel to the mattress is acceptable for most patients. The head should not tilt toward the shoulder or away from it. Stomach sleeping should be avoided entirely when there is confirmed cervical degeneration with nerve root involvement. If changing a lifelong sleeping position sounds impossible, starting with a body pillow on the side to prevent rolling onto the stomach during the night is a practical first step. Changes in morning symptom severity within two to three weeks usually confirm whether the sleeping position was a significant contributing factor.
Section 5: Will It Get Worse? Can It Be Stopped?
31. Is cervical spondylosis reversible, or is this permanent?
Structural reversal of established disc degeneration is not possible. Discs that have lost height do not regain it. Bone spurs that have formed do not dissolve on their own. This is the honest answer, and I give it to every patient. What is reversible, and what I have seen in practice consistently, is the symptom burden. Nerve root inflammation can settle. Muscular strength can be rebuilt. Posture can be corrected. The daily load on compromised structures can be reduced to a level where symptoms resolve even though the structural changes remain visible on MRI. The trajectory of degeneration can be slowed significantly. Patients who address the mechanical causes, correct their posture, strengthen their supporting musculature, and manage their daily loading patterns live well with cervical spondylosis without progressive worsening.
32. Will cervical spondylosis keep getting worse every year regardless of what I do?
Not necessarily. The natural history of cervical spondylosis is not a relentless march toward disability. Many patients reach a point of relative stability where degeneration progresses slowly or plateaus, particularly if the mechanical factors driving it are addressed. The patients who do progress steadily are typically those who continue the same postures and loading patterns that caused the problem, who avoid rehabilitation, or who have additional risk factors like smoking (which reduces disc nutrition), obesity, or significant comorbidities. The spine responds to how it is treated. Change the loading, build the supporting musculature, and the trajectory changes.
33. How do I know if surgery is actually necessary, or if I am being pushed toward it unnecessarily?
Surgery for cervical spondylosis has clear and specific indications. The main ones are: cervical myelopathy, meaning spinal cord compression causing walking problems, hand clumsiness, or progressive neurological deficit; severe radiculopathy with progressive neurological deficit such as worsening arm weakness that does not respond to 6 to 12 weeks of appropriate conservative management; and significant pain with functional disability that has not responded to a genuine conservative trial. Surgery for pain alone, without neurological involvement, is rarely the right first answer. If you have been offered surgery without having had a structured physiotherapy trial, a review of your imaging with a spine specialist who takes time to explain the findings, and a period of anti-inflammatory management, that sequence should happen first. A second opinion from an orthopaedic spine specialist is always appropriate before proceeding with surgery.
34. Can untreated cervical stenosis cause permanent nerve damage?
Yes. This is one of the important distinctions in cervical spondylosis management. Nerve root compression that is causing pain and tingling but no motor weakness is generally reversible with appropriate treatment. Prolonged or severe compression that has caused motor weakness, muscle wasting, or progressive loss of function has a longer and less predictable recovery even after successful decompression. The nerve fibers involved in motor function can sustain permanent damage if compression is sustained at a critical level for long enough. This is why progressive weakness in the arm or hand, new walking problems, or increasing hand clumsiness in a patient with known cervical stenosis is a reason to see a specialist promptly, not to wait and see.
35. Can nutrition, hydration, or vitamin deficiencies affect cervical degeneration?
Yes, and this is genuinely under-discussed in clinical consultations. Intervertebral discs are largely avascular after early adulthood, meaning they receive nutrition by diffusion from the surrounding tissue rather than direct blood supply. Hydration directly affects disc height and resilience. Chronic dehydration accelerates disc desiccation. Vitamin D deficiency is associated with accelerated musculoskeletal degeneration and impairs the ability of muscles supporting the cervical spine to function optimally. Vitamin B12 deficiency produces peripheral nerve symptoms that can overlap with or worsen the symptoms of nerve root compression. Magnesium deficiency contributes to muscle spasm and poor muscle recovery. These are not replacements for mechanical treatment, but they are modifiable factors that affect the pace of degeneration and the quality of the supporting soft tissue environment.
36. Why do some people have severe MRI findings but almost no pain, while others have modest findings but significant disability?
Because the MRI describes the structure, not the nervous system’s sensitivity to that structure. Pain experience is the product of structural pathology plus the nervous system’s sensitivity to signals from that area, plus psychological and contextual factors including sleep quality, stress levels, mood, and prior pain experience. A person with a highly sensitized nervous system from years of chronic pain will experience more disability from the same degree of structural compression than someone who has recently developed similar findings. This is not imaginary pain. It is real pain from real findings, but the same findings produce different experiences in different people. Understanding this helps explain why two patients with similar MRIs have completely different lives, and why psychological factors like sleep restoration and stress management are legitimate parts of cervical spondylosis treatment.
37. Why do symptoms return after a period of relief?
Because the underlying structural changes remain, and the mechanical factors that aggravate them tend to return when people feel better. Patients complete a physiotherapy course, feel significantly improved, return to their previous work patterns and postures, stop their exercises, and then report six months later that symptoms have returned. The structural degeneration has not changed. The behaviors that were loading it have returned. This is why managing cervical spondylosis requires building long-term habits, not completing a finite treatment episode and returning to baseline. The exercises need to continue. The workstation setup needs to remain correct. The phone posture needs to stay at eye level. These are not temporary interventions.
Section 6: The Human Side of This Condition
38. Why do doctors often dismiss neck pain in younger people as stress or anxiety?
Because the clinical guidelines for investigating neck pain are designed around probability, and in younger people, structural cervical degeneration has historically been a lower probability diagnosis than muscular pain or stress-related symptoms. A 25-year-old with neck pain is statistically more likely to have muscular tension than significant spondylosis. The problem is that this statistical logic fails the individual patient whose degeneration is genuinely already present due to years of technology use and postural loading. If your neck pain is mechanical in pattern, worsens with specific positions and screen use, and involves arm symptoms that follow a dermatomal distribution, that pattern needs imaging regardless of your age. Persistent symptoms not explained by simple measures after 4 to 6 weeks deserve proper investigation in any age group.
39. Why do so many patients say “I wish someone had explained this to me earlier”?
Because the gap between what is documented in a clinical record and what a patient actually understands when they leave an appointment is significant. A patient who understands what foraminal narrowing actually means will not perform the movements that compress that foramen. A patient who understands why the cervical curve matters will set their screen at eye level. A patient who knows which symptoms signal nerve root involvement rather than muscle pain will not push through warning signals they should be stopping for. A patient who understands that spondylosis is mechanical and manageable rather than catastrophic will engage with rehabilitation instead of waiting for it to somehow resolve. The explanation is part of the treatment. This page exists because that explanation should have been provided much earlier in most patients’ journeys.
40. Can chronic neck pain affect mental health, and does mental health affect neck pain?
This relationship is bidirectional and clinically important. Chronic pain of any kind significantly increases the risk of depression and anxiety. Sleep disruption from pain compounds this. Social withdrawal from reduced activity adds to it. The pain itself may be modulated by mood, stress levels, and sleep quality through central sensitization mechanisms, meaning the nervous system becomes more broadly sensitized to pain signals when in a state of chronic stress or poor sleep. Addressing sleep, managing stress, and where necessary treating depression or anxiety as part of a comprehensive cervical spondylosis management plan is not a soft add-on. It affects treatment outcomes in a measurable way. None of this means the pain is imaginary. It means the human being experiencing it is more than a cervical spine, and the management needs to reflect that.
About Dr. Prince Uchadiya
Dr. Prince Uchadiya is a DNB Orthopaedics specialist who completed his training at KEM Hospital Mumbai, one of India’s most respected orthopaedic training institutions, and holds a Gold Medal in orthopaedics. He practices at Dr. Prince Uchadiya Orthopaedic And Joint Care Clinic in Indore, with subspecialty expertise in arthroscopy, ligament reconstruction, and joint care. He sees patients with cervical spondylosis as part of a broader spine and musculoskeletal practice that prioritizes explanation, accurate diagnosis, and evidence-based management over rushed consultations and generic prescriptions.
Patients in Indore with cervical spondylosis, neck pain, arm tingling, radiculopathy, or related concerns can consult directly at the clinic. For additional clinical detail on this condition, the complete cervical spondylosis treatment guide covers anatomy, MRI terminology, safe exercises, and the full treatment pathway. For back and spine-related concerns more broadly, the spine and back pain specialist page provides further information on consultations available in Indore. If you are seeking a detailed review of existing imaging or a management plan that has not been working, a structured second opinion is available.


