A patient walked into my clinic last month after twisting his knee during a cricket match in Indore. He had an MRI report in one hand and a confused look on his face. The scan showed a possible partial ACL tear. But before I even opened that report, I placed my hands on his knee and did one thing: the Lachman test. Thirty seconds. No machine. No injection. And I already had 80% of my answer.
That is the power of this one clinical test. It is the single most accurate physical examination technique available for detecting an anterior cruciate ligament injury. Not because it is complicated, but because it is precise, intelligent, and grounded in decades of orthopaedic science.
If your doctor just performed the Lachman test on you, or if your MRI is suggesting an ACL problem and you want to understand what comes next, this guide will walk you through everything. No jargon. No textbook language. Just the kind of explanation a patient deserves.
“The Lachman test is the closest thing we have to a window into the knee. Before the camera, before the scan, your hands tell the truth.”, Dr. Prince Uchadiya, Orthopaedic and Arthroscopic Surgeon, Indore
What the Lachman Test Is Actually Checking Inside Your Knee

To understand this test, you first need to know what the ACL does. The anterior cruciate ligament runs diagonally inside your knee joint, connecting the bottom of your thigh bone (femur) to the top of your shin bone (tibia). Its main job is to stop your tibia from sliding forward. Think of it as an internal rope that keeps your knee stable whenever you change direction, land from a jump, or pivot suddenly.
When that ligament tears, the tibia loses its anchor. It can shift forward with little resistance. This clinical maneuver is designed to detect exactly that shift.
This maneuver works by placing the knee in a slightly bent position, roughly 20 to 30 degrees of flexion, and then gently pulling the tibia forward while holding the thigh still. In a healthy knee with an intact ACL, the shin bone barely moves, and the examiner feels a firm, definitive stop, what clinicians call a “firm endpoint.” In a knee with a torn ACL, the tibia slides forward noticeably, and instead of a firm stop, there is a soft, mushy, or absent endpoint. That softness is the positive finding. That is what changes everything about your diagnosis and treatment plan.
Why the Lachman Test Is More Accurate Than the Anterior Drawer Test Most Doctors Still Use First
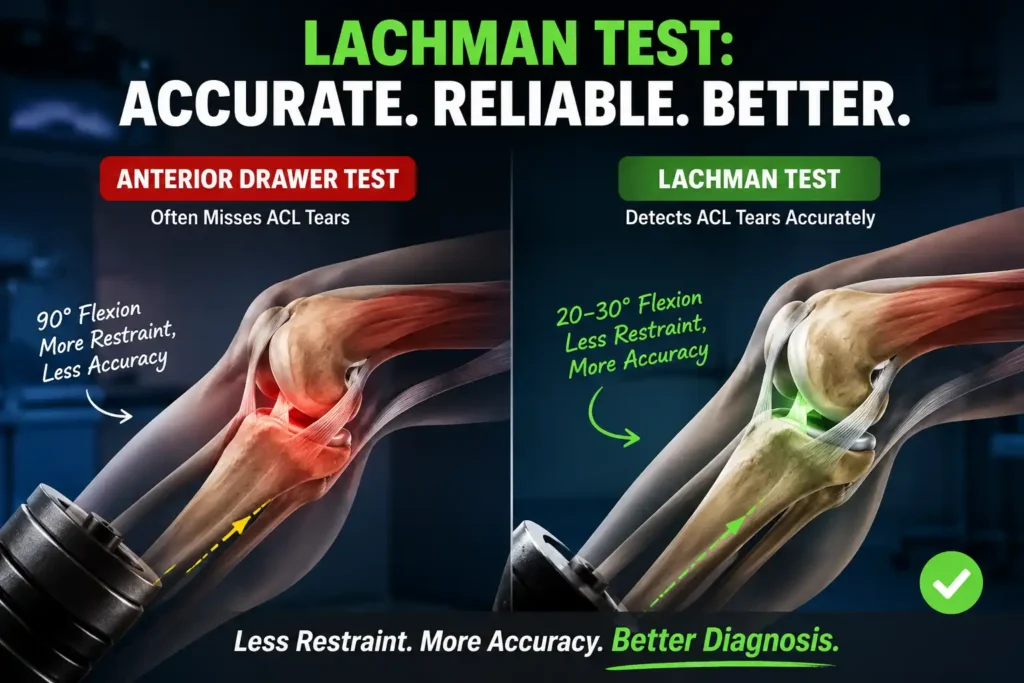
Many patients come to Dr. Prince Uchadiya Orthopaedic And Joint Care Clinic after having another clinical test done elsewhere: the anterior drawer test, where the knee is bent at 90 degrees and the tibia is pulled forward. That test has been the traditional go-to for ACL assessment for decades. But here is the clinical reality.
At 90 degrees of knee flexion, several structures tighten up around the joint: the hamstring muscles, the posterior capsule, the menisci. These structures effectively act as internal brakes, artificially limiting the forward movement of the tibia even when the ACL is completely torn. The result? The anterior drawer test misses a significant number of ACL tears, particularly in the acute phase, when swelling and muscle guarding are at their highest.
This test sidesteps that problem by using a far smaller degree of flexion, 20 to 30 degrees. At this angle, the hamstrings are relaxed, the secondary stabilizers are not yet engaged, and the ACL becomes the primary structure resisting forward tibial translation. This is why the test exposes true ACL insufficiency so much more reliably.
The numbers confirm this clinical logic:
- Lachman test sensitivity: 87% | Specificity: 93%
- Anterior drawer test sensitivity: 48% | Specificity: 93%
- Pivot shift test sensitivity: 61% | Specificity: 97%
Source: NCBI StatPearls: Lachman Test, 2023
The anterior drawer test, for all its historical use, misses roughly half of all actual ACL tears. This test misses far fewer. For a patient sitting anxious in a clinic, that difference is not a statistic: it is a correct diagnosis versus a missed one.
How Dr. Prince Uchadiya Performs the Lachman Test: Step by Step
Understanding the procedure helps patients feel less anxious and helps referring doctors know what to expect from a skilled examiner. Here is exactly how this examination is performed at Dr. Prince Uchadiya Orthopaedic And Joint Care Clinic in Indore:
- Patient positioning: The patient lies flat on their back (supine) on the examination table. The knee being tested is exposed completely.
- Knee angle: The knee is placed in 20 to 30 degrees of flexion. A folded towel or the examiner’s thigh can be placed under the knee to maintain this position comfortably.
- Hand placement: One hand grips the thigh firmly, just above the knee, stabilizing the femur completely. The other hand wraps around the upper tibia, with the thumb resting directly on the tibial tuberosity, the bony bump just below the kneecap.
- The test maneuver: The hand on the tibia applies a smooth, firm, anterior pull forward while the other hand holds the femur absolutely still. This is not a jerky movement. It is controlled, steady, and consistent.
- Reading the result: The examiner evaluates two things: how far the tibia moves, and the quality of the endpoint when movement stops. Both sides of the body are compared. Even 2 mm more movement on the injured side, combined with a soft or absent endpoint, constitutes a positive test.
In clinical practice, a KT-1000 arthrometer can be used to objectively measure the exact millimetres of tibial translation, adding quantitative data to this examination. A difference of more than 3 mm between sides is considered clinically significant.
What a Positive Lachman Test Actually Means for You as a Patient
A positive result does not automatically mean surgery. It means the ACL has lost its structural integrity to a measurable degree, and that demands a proper diagnosis pathway, not a panic response.
When a patient presents with a positive finding, the next steps at Dr. Prince Uchadiya Orthopaedic And Joint Care Clinic follow a logical clinical process:
- Confirm with MRI: A positive clinical test is a strong indicator, but MRI provides definitive structural information: whether the tear is partial or complete, whether the meniscus is involved, and whether other ligaments (PCL, LCL, MCL) were also injured.
- Assess functional demands: A 22-year-old football player in Indore and a 55-year-old office worker have very different activity requirements. The same positive test leads to very different treatment decisions for each.
- Consider associated injuries: ACL tears frequently occur alongside meniscal injuries. Studies show up to 50% of acute ACL tears have a concurrent meniscal injury. During the Lachman test, unusual resistance or catching sensations can sometimes hint at this.
- Grade the laxity: Not all positive tests are equal. Grade 1 means 0 to 5 mm of translation. Grade 2 means 5 to 10 mm. Grade 3 means greater than 10 mm. The grade of laxity helps guide the urgency and type of intervention.
“A positive Lachman test is a starting point, not a sentence. It tells me where to look next and how seriously. In active patients, we take it very seriously, very quickly.”, Dr. Prince Uchadiya
For patients who want to understand the full surgical pathway when ACL reconstruction becomes necessary, read more at our ACL Surgery in Indore page.
When the Lachman Test Can Give a False Negative or a False Positive
No clinical test is perfect. A skilled examiner knows not only how to perform this test but also when to distrust its result. These are the situations where the test can mislead even an experienced clinician:
Situations That Can Cause a False Negative (Missed Tear)
- Acute swelling and pain: In the first 24 to 48 hours after a knee injury, joint swelling and patient guarding can mask tibial translation. The hamstrings tighten involuntarily, artificially stabilizing the joint.
- Chronic ACL rupture: In long-standing tears, the ACL stump can scar down onto the posterior cruciate ligament (PCL) and create a false sense of stability. The knee may not translate forward even though the ACL is functionally absent.
- Examiner experience: This examination is technically demanding. A less experienced examiner may not accurately feel a subtle difference in endpoint quality, especially in large or muscular patients.
- Partial ACL tears: If only one bundle of the ACL is torn, the remaining bundle may still provide enough resistance to mask a true positive finding.
Situations That Can Cause a False Positive (Normal Knee Reading as Torn)
- PCL insufficiency: This is the most important clinical trap. If the PCL is torn, the tibia sits posterior to its normal position. When the Lachman test is performed, the tibia actually returns to its normal position forward, which can be misread as excessive anterior translation.
- General ligamentous laxity: Some patients, particularly hypermobile individuals, have naturally loose ligaments across all joints. Bilateral assessment and comparing both knees together is essential to avoid misinterpreting natural laxity as pathological.
This is why a skilled orthopaedic surgeon never relies on this test in isolation. It is one piece of a complete clinical assessment that includes patient history, mechanism of injury, associated findings, and imaging correlation.
The Lachman Test vs Pivot Shift Test: Why Both Matter in an ACL Workup
Patients sometimes ask why their surgeon performed two or three different knee tests during a single visit. Each test interrogates a different aspect of ACL function, and together they build a more complete picture.
It measures straight-line anterior-posterior instability in a controlled, low-stress position. It is easy to perform awake, reproducible, and highly sensitive for detecting primary ACL insufficiency.
The pivot shift test measures rotational instability: the phenomenon where the tibia suddenly subluxes (shifts forward and inward) and then reduces (snaps back) as the knee goes from extension to flexion. This is the functional instability that makes athletes feel their knee “giving way” during sport. The pivot shift test has higher specificity at 97%, but lower sensitivity at 61%, meaning it catches fewer tears overall but is very specific when it is positive.
In clinical practice, a complete evaluation includes:
- Lachman test: primary assessment of anteroposterior laxity
- Anterior drawer test: supplementary assessment, especially for chronic cases
- Pivot shift test: assessment of rotational instability and functional relevance
- Dial test and varus/valgus stress tests: to rule out associated posterolateral corner and collateral ligament injuries
At Dr. Prince Uchadiya Orthopaedic And Joint Care Clinic, every suspected ACL injury undergoes this complete battery before any decision about MRI sequencing or surgical planning is made.
For patients who need a deeper understanding of what arthroscopic assessment and treatment involves when ACL injury is confirmed, the Arthroscopy Surgery in Indore page explains the full diagnostic and treatment process.
Who Is Most at Risk of a Positive Lachman Test? The Demographics of ACL Tears in Indore
In clinical practice in Indore and across India, ACL tears follow a clear epidemiological pattern. Knowing who is most at risk helps athletes, coaches, parents, and patients recognize when this clinical assessment should be performed urgently rather than waited out.
The highest risk groups include:
- Young male athletes aged 18 to 35: Sports like football, cricket (sudden lateral cuts during fielding), kabaddi, and volleyball all involve the high-deceleration and pivoting movements that put maximum stress on the ACL.
- Female athletes: Females tear their ACL at a rate 2 to 8 times higher than males playing the same sport, due to differences in pelvis width, quadriceps angle, hamstring strength ratios, and hormonal influences on ligament laxity.
- Road traffic accident victims: Dashboard injuries and high-energy knee trauma during accidents are a leading cause of ACL tears in Indian patients, particularly when combined with PCL or MCL injuries.
- Patients who heard a “pop”: A sudden audible pop at the moment of injury, followed by rapid swelling within 2 hours, is one of the most reliable historical indicators of an ACL tear before any physical examination even begins.
According to research published in PMC: Value of Clinical Tests in ACL Diagnosis, the Lachman test demonstrated a sensitivity of 87.6% and specificity of 88.9% in a 2022 study across 165 knee injury patients, confirming its position as the gold standard manual examination for ACL integrity.
What Happens After the Lachman Test at Dr. Prince Uchadiya’s Clinic in Indore
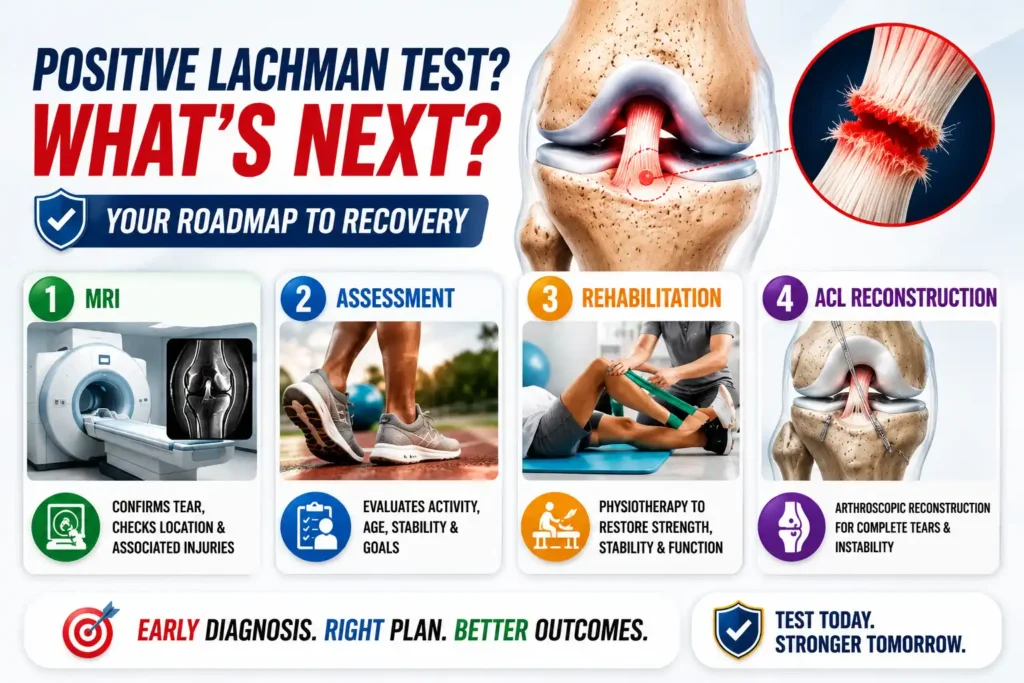
This clinical assessment is the beginning of a conversation, not the end of one. When a patient presents with a positive finding, the clinical pathway at Dr. Prince Uchadiya Orthopaedic And Joint Care Clinic in Nipania, Indore is systematic and structured:
- MRI of the knee: To confirm the tear, classify it (partial vs complete), identify the exact tear location (proximal, mid-substance, or distal), and check for associated meniscal or cartilage pathology.
- Activity and lifestyle assessment: Patients who need ACL reconstruction are identified by their activity level, age, knee stability, and functional demands, not just by the MRI report.
- Non-surgical rehabilitation trial: For partial tears, isolated injuries in older or sedentary patients, or patients who choose to delay surgery, a structured physiotherapy programme focusing on quadriceps and hamstring strengthening can provide functional stability.
- ACL reconstruction: For young, active patients with complete tears and functional instability, arthroscopic ACL reconstruction using hamstring or patellar tendon grafts remains the definitive treatment. Modern keyhole techniques at our clinic allow patients to walk within 2 to 3 weeks and return to sport in 6 to 9 months.
“I have seen patients in Indore walk into my clinic six months after a knee injury, still limping, still managing with a brace, because someone told them it would heal on its own. A complete ACL tear does not heal on its own. The sooner a proper Lachman test and MRI establish the diagnosis, the better the long-term outcome for the joint.”, Dr. Prince Uchadiya
Variations of the Lachman Test You Should Know About
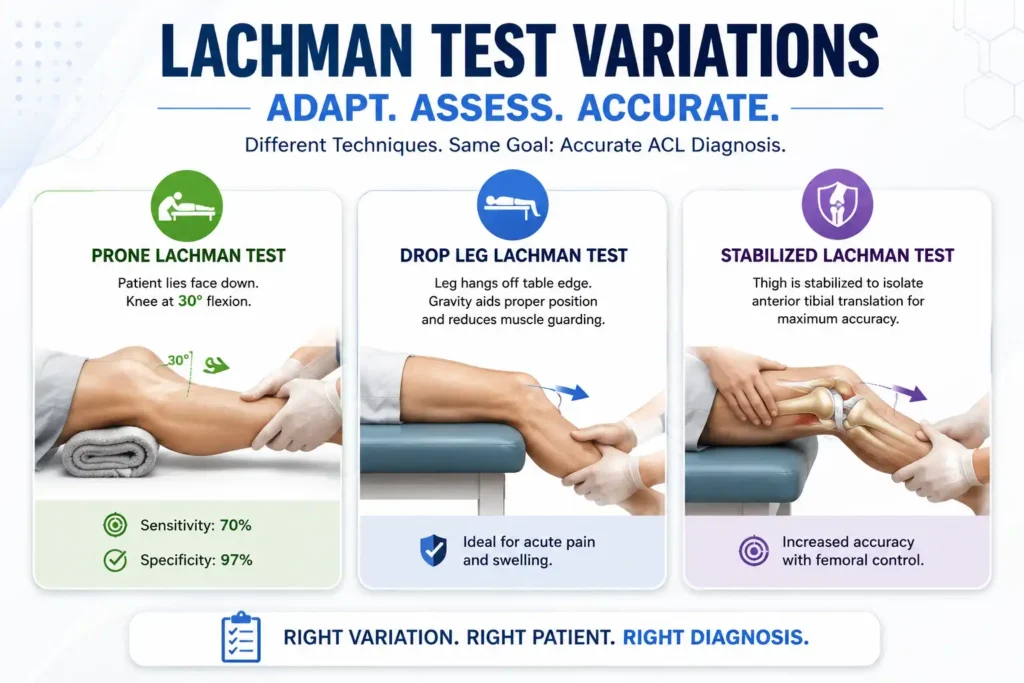
The standard version of this test works well in most settings, but there are clinical situations where modified versions become necessary. Clinicians performing the Lachman test need to adapt based on patient size, patient pain, and examination context.
The Prone Lachman Test
This variation is used when the examiner has smaller hands or when the patient’s thigh is too large to stabilize adequately in the standard supine position. The patient lies face down. The examiner places a rolled towel under the thigh to position the knee at 30 degrees of flexion, then applies forward pressure on the tibia from below. Research published in the Journal of Orthopaedic and Sports Physical Therapy confirmed this variation has 70% sensitivity and 97% specificity, making it particularly useful when initial clinical suspicion is present.
The Drop Leg Lachman Test
The patient lies supine near the edge of the examination table and the leg is allowed to hang slightly off the edge. Gravity naturally positions the knee at the required flexion angle and helps relax the hamstrings, reducing muscle guarding in acute injury settings. This modification is particularly valuable in patients with significant acute swelling or pain who cannot relax sufficiently on a standard examination table.
The Stabilized Lachman Test
Described by Wroble and Linderfeld, this version uses the examiner’s thigh placed underneath the patient’s thigh for better stabilization. Studies prospectively analyzing this technique in 200 acute ACL injury patients found it to be highly sensitive, specific, and accurate, particularly when performed by an experienced orthopaedic surgeon within 30 days of injury.
The One Question Most ACL Patients in Indore Never Ask But Should
After a positive result, most patients ask “Do I need surgery?” That is the right question. But there is a more important question that shapes the answer: “If I do not have surgery now, what happens to my knee in five years?”
The answer is sobering. An unstable ACL-deficient knee does not simply stay the way it is. Every time the knee gives way, every abnormal rotational episode tears a little more of the meniscus and damages the articular cartilage incrementally. A 2023 review in the orthopaedic literature confirms that patients with untreated ACL tears who remain active have significantly higher rates of meniscal tears and early-onset knee arthritis compared to patients who receive timely reconstruction.
This is particularly relevant for young, active patients in Indore who play cricket, kabaddi, football, or who work in physically demanding occupations. This clinical test identifies the problem. What you do with that information determines the long-term health of your knee.
10 Most Asked Questions About the Lachman Test (Real Queries from Patients)
1. Is the Lachman test painful?
In most cases, no. It is a gentle, controlled maneuver. However, if you have significant acute swelling or muscle spasm following a recent knee injury, the test can cause some discomfort. Your doctor will perform it as carefully as possible and will stop if you are in significant pain.
2. Can a Lachman test be negative if I have an ACL tear?
Yes, this is possible. In chronic tears, scar tissue can form between the ACL stump and the PCL, creating false stability. In acute injuries with severe swelling and muscle guarding, the hamstrings can mask tibial translation. A negative result does not completely rule out an ACL tear if clinical suspicion remains high. Always follow with MRI.
3. How long does the Lachman test take?
The actual maneuver takes about 10 to 30 seconds per side. Including bilateral comparison and documentation, the complete evaluation takes 3 to 5 minutes as part of a broader knee assessment.
4. Do I need an MRI if my Lachman test is positive?
In most cases, yes. The clinical finding confirms suspicion of an ACL tear, but MRI is necessary to classify the tear (partial or complete), identify the exact location, check meniscal integrity, and assess cartilage damage. This information is essential for planning treatment.
5. My doctor said my Lachman test has a “soft endpoint.” What does that mean?
A soft endpoint means that when your tibia was pulled forward, it moved without meeting a firm, decisive resistance at the end of its travel. In a healthy knee with an intact ACL, the movement stops with a definite, hard “thud.” A soft endpoint indicates the ACL is not providing that check, strongly suggesting a tear or significant laxity.
6. Can physiotherapy help after a positive test result without surgery?
Physiotherapy cannot repair a torn ACL. However, in cases of partial tears or in patients who are not good surgical candidates, strengthening the quadriceps, hamstrings, and hip stabilizers can compensate partially for ACL insufficiency and improve functional stability. For young, active patients, this is usually a temporary measure rather than a definitive solution.
7. My Lachman test was positive but my MRI says normal. Which do I trust?
This is a genuine clinical dilemma. MRI can occasionally miss partial ACL tears, especially if the ACL stump is intact-looking but functionally incompetent. Clinical examination and MRI must be interpreted together. If the clinical finding is clearly positive with an absent endpoint, your orthopaedic surgeon should take that finding very seriously even if the MRI does not show a complete tear.
8. How is the Lachman test different from the anterior cruciate ligament test done in physiotherapy clinics?
Both physiotherapists and orthopaedic surgeons can perform this evaluation. The technique is identical. What differs is the clinical context: an orthopaedic surgeon integrates the clinical finding with imaging, surgical planning, and reconstruction options, while a physiotherapist typically uses it for ongoing monitoring during rehabilitation. The interpretation and consequences of a positive test depend on who is reading it and in what clinical setting.
9. I heard a pop in my knee during sport. Do I need a Lachman test urgently?
Yes. An audible pop during a sporting activity, particularly during a sudden change of direction or awkward landing, followed by rapid swelling within 2 hours and a feeling of instability, is the classic presentation of an acute ACL tear. You should see an orthopaedic surgeon within 24 to 72 hours for a full clinical examination of ACL integrity. Early evaluation allows timely imaging and prevents further joint damage from weight-bearing on an unstable knee.
10. Is the Lachman test used only for ACL tears or can it detect other knee problems?
This physical examination is designed specifically to evaluate ACL integrity and anterior tibial translation. It is not a general knee examination. However, an experienced examiner may notice additional findings during the test, such as unusual resistance, catching, or crepitus, that suggest concurrent meniscal pathology or cartilage damage. These observations prompt additional specific tests to complete the assessment.