
You wake up at 3am, hand completely numb. You shake it out, the feeling comes back, and you go back to sleep.
This happens again the next night. And the night after that.
A few weeks later you are dropping things without realising it. Your grip has quietly weakened. Typing for more than 20 minutes has become uncomfortable. Holding a phone up to your ear makes the tingling worse.
That pattern, numbness at night, tingling in the thumb and first three fingers, grip loss, and relief from shaking the hand, is the textbook presentation of carpal tunnel syndrome. And it is far more common in Indore than most people realise.
The good news is that carpal tunnel syndrome treatment works extremely well when started at the right time. The problem is that too many people wait until the nerve damage is already significant before they act.
This article covers everything you need to make a smart decision about your own situation.
What Is Carpal Tunnel Syndrome?
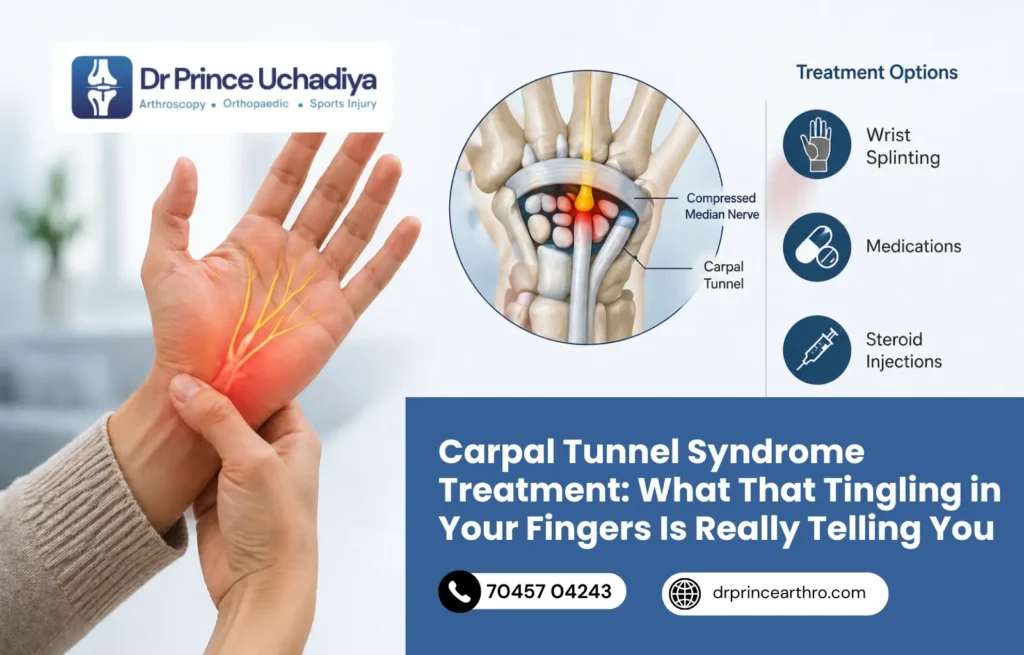
The carpal tunnel is a narrow channel on the palm side of your wrist. It is formed by the wrist bones on the bottom and the transverse carpal ligament across the top.
Running through this tunnel are nine flexor tendons and one critically important nerve: the median nerve.
The median nerve controls sensation in your thumb, index finger, middle finger, and the thumb side of your ring finger. It also controls the small muscles at the base of the thumb that allow you to pinch and grip.
When the space inside the carpal tunnel narrows from swelling, inflammation, fluid retention, tendon thickening, or anatomical factors the median nerve gets compressed. That compression disrupts how the nerve conducts signals. The result is numbness, tingling, pain, and eventually weakness in exactly the fingers the median nerve supplies.
Notice something: your little finger should not be numb in true CTS. The little finger is supplied by the ulnar nerve, not the median. If numbness involves only the little finger, or spreads all the way up the arm, the diagnosis may be something other than carpal tunnel syndrome and needs a different evaluation.
How Common Is Carpal Tunnel Syndrome? The Numbers Are Striking
Carpal tunnel syndrome is the most common focal nerve entrapment disorder in the world, accounting for 90% of all nerve entrapment cases.
According to research published in NCBI StatPearls, the incidence of CTS in the general population ranges from 1% to 5%. In high-risk occupational groups, the prevalence can be far higher.
The gender pattern is unmistakable. CTS affects women at roughly three times the rate of men. In an Indian study from Amritsar, out of 181 female CTS patients, 120 were housewives engaged in repetitive household activities, flour kneading being one of the most commonly cited. The relevance to Indore’s working population is obvious.
Middle-aged adults between 40 and 60 are the most commonly affected group, though it appears in younger people with repetitive wrist-heavy jobs and in pregnant women due to fluid retention in the third trimester.
What Causes It? More Than Just Typing All Day
Carpal tunnel syndrome has a reputation for being a “desk job” condition caused by typing. That is too narrow a picture.
The real cause is sustained or repeated elevation of pressure inside the carpal tunnel, which compresses the median nerve. Many things can create that pressure.
Repetitive Hand and Wrist Movements
Assembly line work, cooking and kneading, carpentry, driving long hours, playing certain musical instruments, using vibrating tools, and yes, prolonged typing or mouse use, all can gradually inflame the tendons running through the carpal tunnel, reducing the space available for the nerve.
Anatomical Factors
Some people simply have a narrower carpal tunnel than others. A wrist-to-thickness ratio above 0.7 is associated with higher CTS risk. This is not something you can change, but it is something that becomes clinically relevant when combined with other risk factors.
Medical Conditions That Change the Tissue Environment
- Diabetes- directly damages nerve sheaths and increases nerve sensitivity to compression
- Hypothyroidism- causes fluid accumulation in soft tissues, including within the carpal tunnel
- Rheumatoid arthritis- causes inflammation of the tendon sheaths inside the tunnel
- Pregnancy- third-trimester fluid retention compresses the median nerve; CTS often resolves after delivery
- Obesity- associated with increased carpal tunnel pressure
Wrist Trauma
A previous wrist fracture, particularly a Colles’ fracture at the distal radius, can change the geometry of the carpal tunnel permanently. CTS appearing years after a wrist fracture is not uncommon, and it is often missed because the connection to the old injury is not obvious.
Sleeping Position
Most people sleep with their wrists flexed. A flexed wrist significantly increases carpal tunnel pressure, which is why nighttime numbness is often the first symptom. The nerve gets compressed for hours while you sleep, and by morning the deficit is obvious.
Carpal Tunnel Syndrome Symptoms: The Progression You Need to Recognise
CTS is a progressive condition. It does not stay mild indefinitely. Understanding the stages helps you act before it becomes harder to treat.
Early Stage
Intermittent tingling and numbness in the thumb, index, and middle fingers, especially at night or during activities that involve sustained wrist flexion like reading, phone use, or driving. Shaking the hand brings relief. This stage is often dismissed as “pins and needles” from an awkward sleeping position.
Moderate Stage
Symptoms become more frequent, appearing during the day too. Pain in the wrist and forearm, sometimes shooting up toward the elbow. Weakness starts showing dropping things, struggling to open jars, losing fine motor precision. Typing becomes uncomfortable after even short sessions.
Severe Stage
Constant numbness that no longer fully resolves with shaking. Visible wasting of the thenar muscles at the base of the thumb. Significant grip weakness. At this point, permanent nerve damage is either beginning or has already occurred. Surgery becomes the primary option, and full recovery is less predictable.
The critical window is the early to moderate stage. Conservative treatment works best here. Surgery at this stage is also highly successful and recovery is faster. Waiting until severe creates a harder problem.
How Carpal Tunnel Syndrome Is Diagnosed in Indore
Diagnosis involves three components working together: the symptom history, the physical examination, and nerve studies.
The Physical Examination Tests
Two clinical tests are used at almost every CTS examination worldwide.
Phalen’s Test: You press the backs of both hands together with fingers pointing downward, holding the wrists in full flexion for 60 seconds. If numbness or tingling appears in the median nerve distribution within that minute, the test is positive. Phalen’s has better sensitivity than Tinel’s for CTS detection.
Tinel’s Sign: The examiner taps over the median nerve at the wrist. A shooting tingling sensation into the fingers is a positive sign. Useful as a marker of nerve irritability, but less reliable than Phalen’s in mild cases.
One important nuance: neither test is definitive on its own. Research confirms that in mild CTS, both tests can be negative even when nerve conduction studies confirm compression. The physical examination provides useful clinical information but requires corroboration.
Nerve Conduction Study and EMG
This is the gold standard for CTS diagnosis. During a nerve conduction study (NCS), small electrodes are placed on the wrist and hand. Mild electrical impulses measure how quickly the median nerve conducts signals across the carpal tunnel.
Slowed conduction velocity or delayed latency at the wrist confirms median nerve compression. The study also grades severity from mild to severe, which directly informs whether conservative treatment or surgery is the better path.
An electromyogram (EMG) adds information about whether the muscles supplied by the median nerve are showing signs of denervation. Significant EMG changes indicate more advanced nerve damage.
Ultrasound of the Wrist
Ultrasound can directly visualise the median nerve inside the carpal tunnel. An enlarged nerve cross-sectional area is a reliable marker of compression. Ultrasound is also used to check for space-occupying lesions (cysts, ganglions) inside the tunnel that might be contributing to the compression.
Carpal Tunnel Syndrome Treatment in Indore: Starting Without Surgery
For mild to moderate CTS, non-surgical treatment is the starting point and it works well for most patients.
Wrist Splinting at Night
A wrist splint holds the wrist in a neutral, slightly extended position during sleep, preventing the flexion that raises carpal tunnel pressure overnight.
Night splinting alone is enough to resolve early-stage CTS in many patients, particularly those whose symptoms are primarily nocturnal. The splint is worn during sleep and during any activity that provokes symptoms. It is simple, non-invasive, and particularly effective during pregnancy-associated CTS.
Activity Modification
Identifying and reducing the specific movements that aggravate the nerve. For someone who types, this means ergonomic adjustments, keyboard height, mouse position, wrist angle during use. For someone whose work involves repetitive gripping or vibration, it means technique changes and more frequent breaks.
This does not mean stopping work. It means working smarter to reduce median nerve irritation during the hours you spend with your hands in use.
Anti-Inflammatory Medication
NSAIDs reduce the inflammatory component contributing to tunnel narrowing. They address the pain and swelling but do not fix the underlying compression mechanism. Useful as part of a combination approach, especially in the acute flare-up phase.
Corticosteroid Injection
A steroid injection directly into the carpal tunnel reduces inflammation around the median nerve rapidly and effectively.
Studies show meaningful short-term relief in the majority of patients, often within days of injection. The effect typically lasts weeks to months. Repeat injections can be given, though the number is limited to avoid tendon weakening from repeated steroid exposure.
Injection is particularly useful as a bridge treatment, giving enough relief to engage in physiotherapy and activity modification while awaiting surgery if conservative management eventually proves insufficient.
Physiotherapy and Hand Exercises
Specific nerve gliding exercises help the median nerve move more freely through the carpal tunnel, reducing adhesions and improving conduction. Tendon gliding exercises keep the flexor tendons supple, reducing their contribution to tunnel pressure.
Physiotherapy is more effective as a complement to splinting and injection than as a standalone treatment in established CTS, but it is a valuable part of the recovery program regardless of whether surgery is eventually needed.
When Surgery Becomes the Right Answer
Surgery for carpal tunnel syndrome is not a last resort born of desperation. It is a straightforward, highly effective procedure with a success rate of 75% to 90% when performed for appropriate indications.
Surgery is indicated when:
- Conservative treatment for 3 to 6 months has not provided adequate relief
- Nerve conduction studies show moderate to severe compression
- EMG reveals signs of denervation in the thenar muscles, indicating motor nerve damage
- Thenar muscle wasting is visible on examination
- Symptoms are severe enough to significantly affect work, sleep, and daily function
- The patient cannot tolerate conservative treatment or has had previous surgery elsewhere on the wrist
One critical point: surgery works better when performed before permanent nerve damage is established. Once the motor fibres are significantly damaged and thenar wasting is visible, surgical decompression can stop progression but may not reverse all the deficit. Early surgical intervention, when indicated, protects long-term hand function.
Carpal Tunnel Release Surgery in Indore: What the Procedure Involves
The operation is called carpal tunnel release. The goal is simple: divide the transverse carpal ligament to enlarge the carpal tunnel and remove pressure from the median nerve.
Two techniques are used:
Open Carpal Tunnel Release
A 2 to 3 cm incision in the palm, directly over the carpal tunnel. The ligament is divided under direct vision. The surgery takes 20 to 30 minutes under local anaesthesia. It is done as a daycare procedure, you go home the same day.
Endoscopic Carpal Tunnel Release
A minimally invasive approach using two small incisions, each about half a centimetre. A camera and a specialised cutting tool are inserted to divide the ligament from the inside, with no incision across the palm. This method results in less palm scar tenderness, faster return to gripping and work, and a better cosmetic outcome.
Recovery from carpal tunnel release surgery is generally straightforward. Most patients begin using the hand for light activities within days. Return to sedentary work happens within 1 to 2 weeks. Return to manual work typically takes 4 to 6 weeks.
Tingling and numbness often begin improving within days of surgery as the nerve is decompressed. Full nerve recovery takes longer, weeks to months depending on how long the compression was present and how advanced the nerve damage was before surgery.
At our clinic in Indore, we perform both open and endoscopic carpal tunnel release as minimally invasive daycare procedures. For patients wanting to understand the broader range of minimally invasive techniques we use, our arthroscopic and keyhole surgery page covers that in detail.
What Happens If You Leave CTS Untreated
This is worth being direct about.
CTS does not stay stable indefinitely. The median nerve, under sustained compression, undergoes progressive changes. The myelin sheath around the nerve fibres degenerates. Axonal injury follows. Muscle fibres begin to waste from lack of nerve supply.
Once the thenar muscles at the base of the thumb have wasted visibly, which happens in severe, long-standing CTS, that wasting is largely irreversible even after surgical decompression. The nerve can regenerate sensation over time, but motor recovery is slower and less complete.
The practical consequences of advanced untreated CTS include permanent grip weakness, inability to pinch or hold objects, difficulty with fine tasks like writing and buttoning clothing, and occupational disability.
For people in Indore whose work involves the hands, from computer workers to cooks to craftspeople, that represents a significant and preventable loss of function.
Jobs in Indore with High Carpal Tunnel Syndrome Risk
Occupational exposure is one of the strongest predictors of CTS development. In Indore’s specific work environment, several roles carry above-average risk:
- IT and software professionals who spend 6 to 10 hours a day at a keyboard
- Garment and textile workers performing repetitive stitching and cutting motions
- Cooks and caterers involved in sustained kneading, chopping, and stirring
- Auto mechanics and factory workers using vibrating tools
- Delivery and logistics drivers holding steering wheels for extended periods
- Home-based workers involved in traditional crafts and domestic tasks
For anyone in these occupations with wrist or hand symptoms persisting beyond 2 weeks, an early assessment is worthwhile. The earlier CTS is identified, the more treatment options are available and the more reversible the nerve changes are.
Dr. Prince Uchadiya’s Perspective on Carpal Tunnel Syndrome
Carpal tunnel syndrome is one of the conditions where the gap between how simple the treatment is and how long patients wait before getting it is most striking.
People tolerate the nighttime numbness for months, sometimes years, before coming in. By that point, some have developed thenar wasting. They have lived with a treatable condition for so long that the nerve has begun to give up on that territory.
The diagnosis is not complicated. A good clinical examination plus a nerve conduction study gives you the full picture in a single appointment. And treatment at the early or moderate stage is straightforwar, splinting and activity modification for many, injection for those with more persistent pain, and surgery for those who need it. Surgery itself takes less than half an hour and patients go home the same day.
What I tell every patient: the nerve is sending you signals. The tingling at night, the hand waking you up, the grip going, these are not things to manage and accept as normal. They are the median nerve under pressure asking for help. The sooner you act, the more completely we can get you back to a normal functioning hand.
If you are in Indore and recognise even one or two of the symptoms in this article, come in for an evaluation. An accurate assessment takes one consultation. Letting it drift for another year does not.
Visit the Dr. Prince Uchadiya Orthopaedic And Joint Care Clinic to book a consultation or learn more about our approach to hand and wrist conditions.
10 Frequently Asked Questions About Carpal Tunnel Syndrome Treatment
1. What are the first signs of carpal tunnel syndrome?
The earliest signs are typically intermittent numbness and tingling in the thumb, index, and middle fingers, especially at night or after activities involving sustained wrist flexion. Shaking the hand out brings temporary relief. Many people also notice that holding a phone, book, or steering wheel for more than a few minutes triggers the tingling. If these symptoms have been present for more than two weeks, an assessment is worthwhile.
2. Can carpal tunnel syndrome heal on its own?
Mild CTS, particularly when caused by temporary factors like pregnancy or an acute wrist sprain, can resolve spontaneously once the underlying cause resolves. CTS driven by repetitive occupation, anatomical narrowing, or medical conditions like diabetes or hypothyroidism does not resolve without treatment. Without intervention, it typically progresses to more significant nerve damage over time.
3. Is surgery always needed for carpal tunnel syndrome?
Not always. Conservative treatment including night splinting, activity modification, and corticosteroid injection is effective for many patients with mild to moderate CTS. Surgery is reserved for cases where conservative treatment has failed after 3 to 6 months, where nerve conduction studies show significant damage, or where thenar muscle weakness or wasting is already present.
4. How long does carpal tunnel surgery recovery take?
Recovery from carpal tunnel release is faster than most patients expect. Light hand use resumes within days. Return to desk work typically happens within 1 to 2 weeks. Return to manual or labour-intensive work takes 4 to 6 weeks. Full nerve recovery, including complete resolution of tingling and strength restoration, takes weeks to months depending on how long the nerve was compressed before surgery.
5. What is the success rate of carpal tunnel surgery?
Long-term research shows a success rate of 75% to 90% for carpal tunnel release surgery, with most patients reporting significant improvement in numbness, tingling, and hand function. Outcomes are better when surgery is performed before permanent motor nerve damage occurs. For patients who have already developed thenar wasting, sensory recovery is still likely, but full motor recovery is less predictable.
6. Does carpal tunnel syndrome affect both hands?
Yes. CTS is bilateral in a significant proportion of patients, though it often starts more severely on one side. The dominant hand is frequently affected first, but both hands should be assessed in any patient presenting with CTS symptoms. Bilateral CTS can sometimes indicate an underlying systemic condition like diabetes or hypothyroidism that is affecting both peripheral nerves simultaneously.
7. What tests are done to diagnose carpal tunnel syndrome?
Diagnosis involves a clinical examination including Phalen’s test and Tinel’s sign, followed by a nerve conduction study (NCS) and electromyogram (EMG). The NCS measures how quickly the median nerve conducts signals across the wrist, slower than normal confirms compression. The EMG detects whether the thenar muscles are showing signs of denervation. Ultrasound of the wrist can directly visualize the enlarged median nerve inside the tunnel. Together, these tests confirm the diagnosis and grade its severity. Our clinic in Indore offers comprehensive assessment including clinical examination and arrangement of relevant nerve studies.
8. Can carpal tunnel syndrome be caused by a previous wrist fracture?
Yes. A wrist fracture, particularly at the distal radius, can alter the geometry of the carpal tunnel permanently or cause scar tissue formation that narrows the available space for the median nerve. CTS appearing months to years after a wrist injury is well recognised and should be considered in anyone with a history of wrist trauma and new-onset hand numbness or tingling. Our fracture management expertise means we are well positioned to assess these combined presentations.
9. Are wrist splints effective for carpal tunnel syndrome?
Yes, particularly for early-stage CTS and for nocturnal symptoms. A properly fitted wrist splint keeps the wrist in a neutral position during sleep, preventing the flexion that raises carpal tunnel pressure and compresses the median nerve overnight. Splints are also helpful during activities that provoke symptoms. They are most effective in mild cases and during pregnancy-related CTS, where symptoms often resolve fully after delivery.
10. How do I know if my hand numbness is carpal tunnel syndrome or something else?
The distribution of numbness is the first clue. True CTS affects the thumb, index finger, middle finger, and thumb side of the ring finger, the median nerve territory. Numbness involving only the little finger suggests ulnar nerve involvement rather than CTS. Numbness in all fingers spreading up the arm could indicate a neck or cervical spine problem rather than a wrist issue. Numbness on the back of the hand also points away from CTS, which primarily affects the palm-side fingers. A clinical examination by an orthopaedic specialist combined with a nerve conduction study will give a definitive answer. Come in for a proper assessment at our Indore clinic, the diagnosis changes the treatment completely.


